You're often seeing it before you have a name for it.
A client sits with their back to the wall. Their eyes move to the door each time someone passes. A dropped folder in the hallway makes them flinch. During testimony prep, they lose their train of thought when a knock interrupts the meeting. In the file, these moments can look minor. In a forensic evaluation, they can be clinically meaningful.
For immigration attorneys, that distinction matters. In asylum, VAWA, T Visa, and U Visa matters, hypervigilance may help explain why a client avoids certain places, gives fragmented testimony, mistrusts authority, or appears guarded even in a safe office. It can support nexus, credibility analysis, hardship narratives, and functional impairment, but only if it's described with precision and documented in a way that fits evidentiary standards.
What is hypervigilance, then? Not just “being nervous.” Not a personality trait. Not a diagnosis by itself. It is better understood as a trauma-related pattern of sustained threat monitoring that affects attention, physiology, behavior, and daily functioning. For legal strategy, the key question isn't just whether a client feels afraid. It's whether their mind and body are still acting as if danger is nearby, and whether that pattern can be observed, elicited, and tied to the events at issue in the case.
Table of Contents
- Defining Hypervigilance Beyond 'Feeling Jumpy'
- The Neurobiology of a Brain on High Alert
- Observable Signs and Symptoms in Clients
- Distinguishing Hypervigilance from General Anxiety
- Documenting Hypervigilance for Immigration Cases
- Impact on Daily Life and Courtroom Testimony
- Effective Treatment and Management Strategies
- Frequently Asked Questions for Legal Professionals
Defining Hypervigilance Beyond 'Feeling Jumpy'
A useful analogy is a smoke alarm that became too sensitive after a fire. It was installed to protect the home. It did its job. But after enough exposure to danger, it starts reacting to steam, toast, or harmless noise. Hypervigilance works much the same way. The person isn't choosing to overreact. Their threat-detection system is firing too often and too fast.
That's why what is hypervigilance is a legal as well as clinical question. If an attorney treats it as simple nervousness, the record stays shallow. If it's understood as a persistent state of heightened alertness, the attorney can ask better questions, frame client behavior more accurately, and recognize when a psychological evaluation may add probative value.
What it looks like clinically
Hypervigilance usually shows up as persistent scanning, exaggerated attention to sound or movement, difficulty settling physically, and a readiness for threat that doesn't turn off when the setting is safe. Clients may monitor entrances, track who is behind them, or react strongly to small disruptions.
That pattern matters because it often exists even when the person can't explain it well. Some clients say only that they feel “tense” or “can't relax.” Others deny feeling anxious while their body tells a different story.
Practical rule: Don't rely only on the client's label for the symptom. Watch what they do with their eyes, posture, breathing, and attention during the interview.
Why “jumpy” is too imprecise
A controlled study of 71 participants found that people assigned to a hypervigilant condition showed changes in visual scanning and autonomic arousal even though their self-reported anxiety did not differ from comparison conditions, as reported in this controlled study on measurable hypervigilance patterns. That finding is foundational. It shows hypervigilance can be observed as an attentional and physiological pattern, not just described as a feeling.
For legal purposes, that distinction helps in two ways:
- It supports objective framing. The symptom can be documented through behavior and clinical observation, not only through self-report.
- It explains apparent inconsistencies. A client may minimize distress verbally while still presenting with clear signs of heightened arousal.
- It strengthens trauma interpretation. The issue isn't merely fearfulness. It's a nervous system that remains organized around threat detection.
Attorneys often worry that describing hypervigilance sounds too abstract. It doesn't have to. In a declaration or evaluation, the strongest language is concrete: the client sat facing the exit, startled when the door opened, repeatedly checked the window, and needed time to reorient after hallway noise. Those are not dramatic embellishments. They are behavioral facts.
The Neurobiology of a Brain on High Alert
Hypervigilance is easier to explain to a court when you translate the science into one simple proposition. The brain has started treating uncertainty as possible danger. Once that happens, neutral events don't stay neutral for long.
Early in an evaluation, I often see the legal consequence of that process. The client isn't merely worried about what might happen next week. They are monitoring what is happening right now. Footsteps outside the office. A chair scraping in the hall. A question asked in a formal tone. Their attention keeps shifting because their brain is ranking possible threat above conversation.
A visual summary can help make that mechanism easier to grasp.
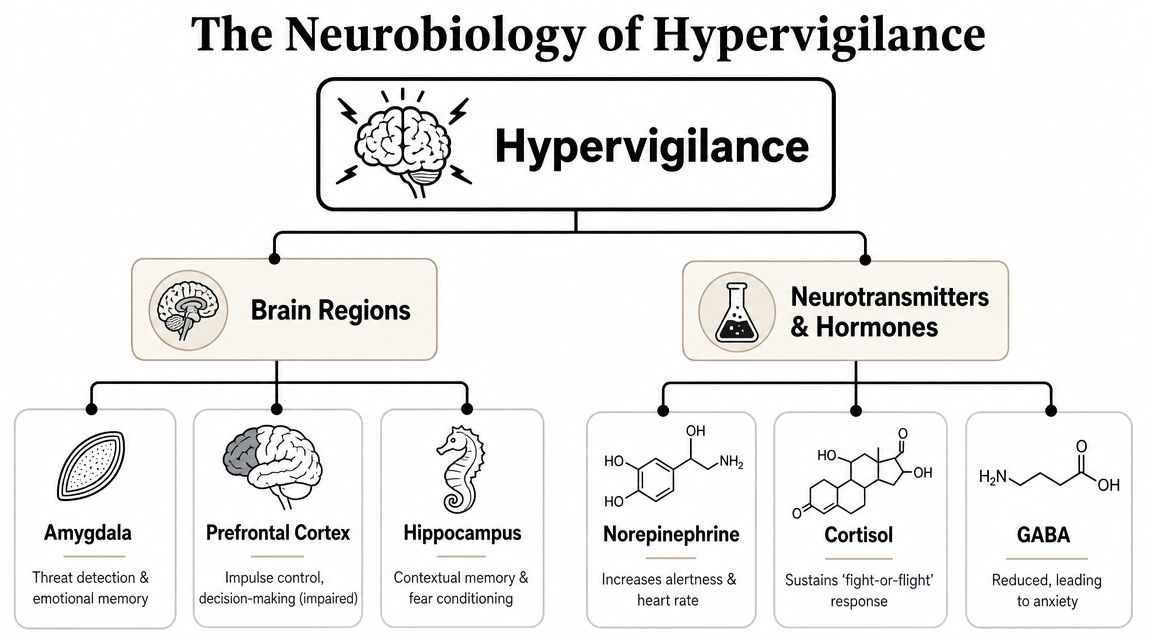
Threat detection, not overthinking
Hypervigilance is best understood as a threat-detection bias in which the nervous system remains in a chronically heightened alert state. Research has linked that pattern to overactive salience-network signaling, and neuroimaging literature reports exaggerated amygdala reactivity to ambiguous or neutral cues, meaning the brain may treat uncertainty as danger, as discussed in this review of hypervigilance, salience processing, and amygdala reactivity.
That's the core mechanism attorneys need. A hypervigilant client doesn't need an objectively dangerous room to feel activated. Ambiguity is enough.
Here is a brief video explanation that can help attorneys and advocates think about the underlying biology in plain terms.
Why this matters to legal strategy
In immigration cases, the neurobiology helps answer a question adjudicators often ask implicitly: why is the client still reacting this way if they are now in the United States, in counsel's office, or in a courtroom with formal protections?
Because the nervous system doesn't reset on command. A client can know intellectually that your office is safe and still react physiologically as if they need to prepare for danger. That gap between knowledge and bodily response is common in trauma presentations.
A client may trust counsel and still keep scanning the room. Those facts don't conflict. They describe different systems operating at the same time.
This also has evidentiary value when testimony seems fragmented. Continuous threat monitoring pulls attention away from task-focused processing. In plain English, the client may be trying to answer accurately while part of their mind remains occupied with watching, listening, and bracing. That can slow recall, disrupt sequencing, and make testimony appear uneven.
The practical trade-off is straightforward. If counsel ignores the biology, the client may be judged as evasive or inconsistent. If counsel understands it, the same behavior can be contextualized as a trauma-related attentional burden that affects presentation without implying deception.
Observable Signs and Symptoms in Clients
Attorneys usually don't need to diagnose hypervigilance. They do need to recognize it. The most useful approach is to sort what you see and hear into physical, behavioral, emotional, and cognitive signs. That keeps your notes concrete and makes referrals more targeted.

Signs you can observe in the room
Some indicators appear before you ask a single trauma question.
- Physical presentation can include visible tension, shallow breathing, a strong startle to routine office noise, restless posture, or difficulty remaining settled in the chair.
- Behavioral patterns often include sitting near the exit, checking the door repeatedly, scanning the hallway, reluctance to enter crowded waiting rooms, or asking who else can hear the conversation.
- Emotional shifts may look like irritability, abrupt fear, guardedness, or disproportionate distress after a minor interruption.
- Cognitive strain can show up as distractibility, losing track of the question, racing interpretations of neutral events, or trouble concentrating when the environment changes.
These aren't diagnostic by themselves. They are observations that may support a trauma-informed hypothesis.
Questions that produce useful answers
Broad questions usually get broad answers. Specific questions produce better testimony preparation and better forensic referrals.
Try prompts like these:
- Environment-based questions such as “Where do you prefer to sit in public places?” or “What do you notice first when you enter a room?”
- Startle questions such as “What happens in your body when you hear sudden noise?” or “Do interruptions make it hard to keep talking?”
- Safety behavior questions such as “Do you avoid crowds, public transportation, police presence, or unfamiliar buildings?”
- Attention questions such as “When you're talking to someone, do you stay focused on them or keep tracking what's happening around you?”
The strongest observations are small and specific. “Client repeatedly looked at the door during the interview” is more useful than “client seemed anxious.”
What doesn't work is overinterpreting every guarded behavior as trauma. Some clients are cautious because of culture, prior legal experiences, shame, language barriers, or fear of confidentiality breaches. Hypervigilance becomes more persuasive when multiple signs cluster together and fit the client's trauma history.
Distinguishing Hypervigilance from General Anxiety
This distinction is where many legal records get muddled. A declaration may say the client is “always anxious,” but that phrase can flatten an important difference. Hypervigilance is usually organized around scanning for external threat. Generalized anxiety is more often organized around diffuse worry, anticipation, and internal rumination. They can coexist, but they aren't the same thing.
That difference matters in immigration law because hypervigilance often supports a narrative tied to prior persecution, abuse, trafficking, or victimization. When the symptom is accurately described, it helps connect present functioning to past events. When it's misnamed, the case can lose specificity.
Why diagnosis language matters
Cleveland Clinic notes that hypervigilance is not a diagnosable mental health condition and may occur with PTSD, anxiety disorders, personality disorders, and even physical conditions such as hypothyroidism, as explained in this clinical overview of hypervigilance and differential diagnosis. For attorneys, the practical point is simple. Don't present hypervigilance as a standalone diagnosis. Present it as a symptom that must be interpreted in context.
That context affects the weight of the evidence. If a client has trauma exposure and a pattern of threat scanning, a clinician may conceptualize hypervigilance within PTSD or another trauma-related formulation. If the same behavior appears without clear trauma linkage, the analysis may look different.
Hypervigilance and generalized anxiety compared
| Feature | Hypervigilance (Symptom of PTSD) | Generalized Anxiety (Disorder) |
|---|---|---|
| Primary focus | External threat monitoring | Ongoing worry across multiple domains |
| Attention pattern | Scans surroundings for danger cues | Returns to feared possibilities and future outcomes |
| Common trigger style | Reminders of past harm, authority, uncertainty in the environment | Uncertainty about health, work, family, finances, or daily life |
| In-session presentation | Watches doors, startles, tracks noise, guards physical position | Seeks reassurance, worries verbally, anticipates bad outcomes |
| Legal relevance | Often supports trauma nexus and explains courtroom behavior | May explain distress but doesn't by itself establish trauma linkage |
| Diagnostic status | Symptom, not a standalone diagnosis | Formal mental health disorder when criteria are met |
The mistake to avoid
The biggest mistake is treating all distress as interchangeable. If a client says, “I can't stop worrying,” the attorney should ask whether the worry is mostly about future outcomes or whether the client is constantly checking the environment for danger. Those are different clinical pathways.
Forensic reports should reflect that difference clearly. Precision helps the court understand why the symptom matters, how it arose, and what inferences should not be drawn from the client's presentation.
Documenting Hypervigilance for Immigration Cases
Good documentation doesn't begin with a conclusion. It begins with method. If hypervigilance is going to matter in an asylum, VAWA, T Visa, or U Visa case, the record should show how the clinician reached the opinion, what behaviors were observed, and why those findings are relevant to the legal questions in the matter.
Start with history, not labels
A reliable evaluation first clarifies exposure history. What threats did the client face. Were they repeated, unpredictable, targeted, or authority-related. Did the client have to stay alert to avoid harm. Those questions matter more than asking, “Are you hypervigilant?”
Then the evaluator examines temporal sequence. Did the scanning, startle, avoidance, and sleep disruption emerge after the abuse, persecution, trafficking, or crime? If the timing fits, the symptom is easier to connect to the events that ground the legal claim.
For attorneys, a trauma-informed assessment approach is especially useful because it reduces the risk of shallow interviewing that either misses trauma symptoms or elicits them in a chaotic, unreliable way.
Behavioral observations that courts can understand
Behavioral notes are often more persuasive than abstract descriptors. A strong report may document facts such as these:
- Entry behavior such as pausing before entering, checking windows, or asking about privacy.
- Seat selection such as preferring a chair near the door or resisting a seat with their back exposed.
- Reactivity during interview including visible startle when someone knocks, turning toward hallway sounds, or needing extra time to resume after interruption.
- Speech and concentration such as losing track of chronology when environmental stimuli compete for attention.
These observations shouldn't be theatrical. They should be accurate, restrained, and tied to the clinical formulation.
Courts tend to trust symptom descriptions when they read like field notes, not advocacy slogans.
Corroboration and forensic discipline
A defensible report usually integrates several layers of information:
- Clinical interview data that identifies trauma exposure, symptom development, and functional impact.
- Direct observation during the evaluation.
- Testing and symptom measures where appropriate, interpreted cautiously and in context.
- Collateral consistency with declarations, affidavits, medical records, shelter records, police records, or treatment notes when available.
This is also where case strategy becomes concrete. Hypervigilance may help explain delayed disclosure, fear of officials, fragmented memory under stress, inability to remain in shared housing, or distress around surveillance and authority. But the evaluator must still draw the line carefully. The report should explain the symptom's significance without pretending it proves every disputed fact in the case.
One option attorneys use is Pro Psychological Analysis, which provides immigration-focused psychological evaluations and reports for matters such as asylum, VAWA, T Visa, U Visa, and hardship cases. The value of any evaluator, however, depends on methodological clarity, careful interviewing, and writing that translates clinical findings into legally understandable conclusions.
What doesn't work is a thin letter stating only that the client “has PTSD symptoms including hypervigilance.” That language is too conclusory. USCIS officers and immigration judges need the pathway from event to symptom to function. Without that chain, the term adds little.
Impact on Daily Life and Courtroom Testimony
Hypervigilance isn't important because it sounds clinical. It's important because it changes how a person lives and how they appear when they're asked to tell their story under pressure.
Consider a client who cannot ride public transportation because enclosed, crowded spaces make them feel exposed. Another can't keep a restaurant job because every shout from the kitchen pulls their attention away from tasks. A parent becomes irritable at home because their body never exits alert mode, and ordinary household noise feels like a warning signal. Those patterns can support hardship, explain instability, and illuminate why functioning remains impaired long after the precipitating events.
Functional cost outside the legal setting
In a Chicago-based study, people in the highest quartile of hypervigilance had an adjusted 8.6 mmHg higher blood pressure than those in the lowest quartile. The same study found that exposure to police violence was associated with a 9.8-percentage-point increase in hypervigilance scores on a 100-point scale, and among participants who had experienced a police stop, describing it as traumatic was associated with a 20.0-percentage-point increase, as reported in this study of hypervigilance, police violence, and blood pressure.
That doesn't mean every client with hypervigilance will present with the same medical effects. It does show that the symptom is tied to real-world exposure and physiological burden, not just subjective discomfort.
Why testimony can look misleading
In court or at interview, hypervigilance can distort presentation in ways adjudicators may misread.
- Distracted appearance may reflect constant monitoring of the room, not indifference.
- Delayed answers may reflect interruption of concentration by perceived threat cues.
- Guarded eye contact may reflect survival habits around authority, not evasiveness.
- Emotional surges may follow a trigger in the room rather than a dishonest answer.
A client who keeps glancing at the door during cross-examination may look suspicious to someone unfamiliar with trauma. In context, that same behavior may be entirely consistent with a nervous system primed to detect intrusion.
When a courtroom activates threat monitoring, demeanor becomes a poor proxy for truthfulness.
That has practical consequences for preparation. Attorneys may need to slow pacing, explain room layout in advance, reduce unnecessary interruptions during prep, and alert the trier of fact that trauma symptoms can affect presentation. The point isn't to excuse contradictions. It's to prevent trauma-driven behavior from being mistaken for deceit.
Effective Treatment and Management Strategies
Hypervigilance can improve, but it usually doesn't respond well to advice like “just relax” or “try not to think about it.” Those instructions fail because the problem isn't only cognitive. It's physiological, attentional, and often conditioned by trauma.
What tends to help
Treatment is generally strongest when it addresses both trauma meaning and nervous system regulation. Depending on the client's history and diagnosis, that may include trauma-focused psychotherapy, EMDR, skills-based work on grounding and arousal reduction, and psychiatric consultation when clinically indicated.
For clients who are already in treatment or considering it, attorneys may find it helpful to understand how approaches like EMDR for complex trauma are discussed in trauma care settings. The legal relevance is modest but real. Consistent treatment can show effort toward stabilization and may improve the client's ability to participate in the case.
Short-term tools for legal proceedings
A few practical strategies can help before interviews, evaluations, or hearings:
- Grounding through orientation by naming the date, location, exits, and who is present in the room.
- Sensory regulation such as feeling both feet on the floor, holding a cool object, or focusing on controlled breathing.
- Pacing disclosures so the client doesn't move from neutral history straight into the most traumatic events without preparation.
- Break planning that allows the client to reset after visible activation.
No single technique resolves hypervigilance on the spot. The realistic goal is better regulation, not instant calm. For legal teams, even modest improvement can make communication more reliable and reduce the chance that the process itself worsens the symptom pattern.
Frequently Asked Questions for Legal Professionals
Quick answers attorneys can use
| Question | Answer |
|---|---|
| Is hypervigilance a diagnosis by itself? | No. It's better understood as a symptom that appears in context and requires differential diagnosis. |
| Can hypervigilance support an asylum, VAWA, T Visa, or U Visa case? | Yes, when it is carefully linked to the client's trauma history, observed behavior, and current functional impairment. |
| Does a client need to use the word “hypervigilance” for it to matter? | No. Many clients describe behavior and body reactions without knowing the clinical term. |
| Can hypervigilance affect credibility assessments? | It can affect demeanor, concentration, pace, and emotional expression. Those effects shouldn't be confused with fabrication. |
| Should attorneys diagnose it themselves? | No. Attorneys should document observations, ask focused questions, and seek a qualified evaluation when the symptom may be legally significant. |
| What kind of interview helps clarify it? | A structured, trauma-informed interview is often more reliable than casual conversation. Attorneys who want a better framework may find this overview of structured interviewing in psychological assessment useful. |
A few final practice points are worth keeping in mind.
First, don't overstate the symptom. Hypervigilance is powerful evidence when it's described carefully and tied to facts. It loses value when it's used as a catch-all explanation for every difficulty in the record.
Second, don't ignore it because it seems subtle. Some of the most persuasive trauma evidence comes from ordinary observations made consistently: where the client sits, what interrupts their attention, how they react to noise, and whether their body ever appears at ease.
Third, remember the legal function. The goal isn't to produce clinical vocabulary for its own sake. The goal is to help the adjudicator understand why this client behaves as they do, how the symptom connects to past harm, and why that pattern belongs in the evidentiary picture.
When hypervigilance is affecting a client's history, functioning, or testimony, a careful forensic evaluation can make the record clearer and more clinically precise. Pro Psychological Analysis provides psychological evaluations for U.S. immigration cases, including reports that document trauma-related symptoms in a format attorneys can use in asylum, VAWA, T Visa, U Visa, and hardship matters.