Most advice about complex PTSD EMDR is too neat for the cases immigration attorneys encounter. It treats EMDR as if the therapist identifies one bad event, runs a standard protocol, and the client quickly becomes calmer, more consistent, and easier to present in a declaration or hearing. That picture is incomplete, and in some cases unsafe.
For survivors of trafficking, domestic violence, torture, detention, childhood abuse, or repeated coercive control, trauma usually isn't stored as one clean narrative. It tends to show up as fragments, body reactions, shame themes, missing pieces, and abrupt shifts in emotional state. In legal practice, that matters. A client may look evasive when they are dissociating, inconsistent when they are retrieving memory by fragments, or detached when they are trying not to become overwhelmed.
EMDR deserves its place in serious trauma treatment. The U.S. Department of Veterans Affairs and Department of Defense describe it as one of the most studied PTSD treatments, with a large body of research showing it is effective when delivered over roughly 3 months, typically in weekly sessions up to 90 minutes, and note that it holds the strongest recommendation status in several PTSD clinical practice guidelines (VA and DoD guidance on EMDR for PTSD). But that same credibility is exactly why attorneys should resist oversimplified marketing. A strong treatment can still be poorly timed, poorly adapted, or poorly documented.
In immigration cases, the question usually isn't just whether EMDR can help. Key questions are whether it's indicated now, whether the clinician understands complex trauma, and whether treatment records can support the legal narrative without overstating what therapy can prove. Good clinical work and good forensic documentation are related, but they aren't the same thing.
Table of Contents
- EMDR for Complex PTSD An Introduction
- Understanding Complex PTSD Beyond a Simple Diagnosis
- How EMDR Therapy Reprocesses Traumatic Memories
- Adapting the EMDR Protocol for Complex Trauma Survivors
- Reviewing the Evidence and Managing Outcome Expectations
- Essential Safety Protocols and When to Postpone EMDR
- Translating EMDR Treatment into Persuasive Legal Evidence
EMDR for Complex PTSD An Introduction
The common legal mistake is to treat EMDR as a speed tool. Attorneys hear that a client can start treatment, process trauma, and then give a cleaner statement. In complex PTSD cases, that assumption can damage both the treatment and the case record.
EMDR can be appropriate for complex trauma. The forensic question is different. Counsel needs to know whether the treatment is being paced in a way that protects the client, and whether the record will later show a clinically sound basis for changes in recall, affect, and functioning.
Complex PTSD shifts the objective. The issue is rarely one isolated event with one clean target memory. The clinician is often dealing with a layered pattern of coercion, captivity, assault, betrayal, and chronic threat that changed how the client encodes experience and responds under stress. In asylum, VAWA, T visa, and U visa cases, that difference matters because the treatment notes may become part of the evidentiary story.
A useful comparison is burn care versus treating a cut. With a single incident trauma, the clinician may focus on a discrete memory network. With complex trauma, the work often involves multiple linked networks, each connected to a trigger set, bodily response, belief system, and relationship pattern. That affects how quickly EMDR can proceed and what progress looks like in the file.
Early progress is often modest but legally important. The client may stay oriented longer during preparation meetings. Panic may become more predictable. Shame-based avoidance may lessen enough for the person to discuss categories of abuse without fragmenting. Those changes can improve interview reliability, but they do not guarantee tidy chronology or complete recall.
For case strategy, attorneys should avoid using symptom reduction as a proxy for credibility. A better question is whether treatment records document a consistent clinical process: target selection, stabilization work, dissociation screening, reprocessing attempts, interruptions, and the client's response. That kind of documentation helps explain why testimony may become clearer in some areas, remain incomplete in others, and fluctuate under stress.
Mainstream recognition of EMDR still matters in this setting, as noted earlier. It helps establish that the clinician selected a well-accepted trauma treatment rather than an improvised method. The stronger forensic point, though, is not that EMDR exists in treatment guidelines. It is that the therapist adapted it responsibly for complex trauma and documented those adaptations in a way a court or adjudicator can follow.
In practice, the difference between useful EMDR records and weak ones usually comes down to four things: whether the clinician identified the relevant trauma pattern, whether stabilization preceded intensive processing, whether sessions noted dissociative responses or other barriers, and whether the chart connects treatment events to observed functional change. That is the level of detail that helps an immigration attorney use clinical evidence without overstating what therapy can prove.
Understanding Complex PTSD Beyond a Simple Diagnosis
Complex PTSD is less like one wound and more like a pattern of injuries that changed how the person learned to survive. In legal settings, reducing it to a symptom checklist misses the point. What the attorney needs to understand is how the condition affects memory, behavior, trust, and day-to-day functioning.
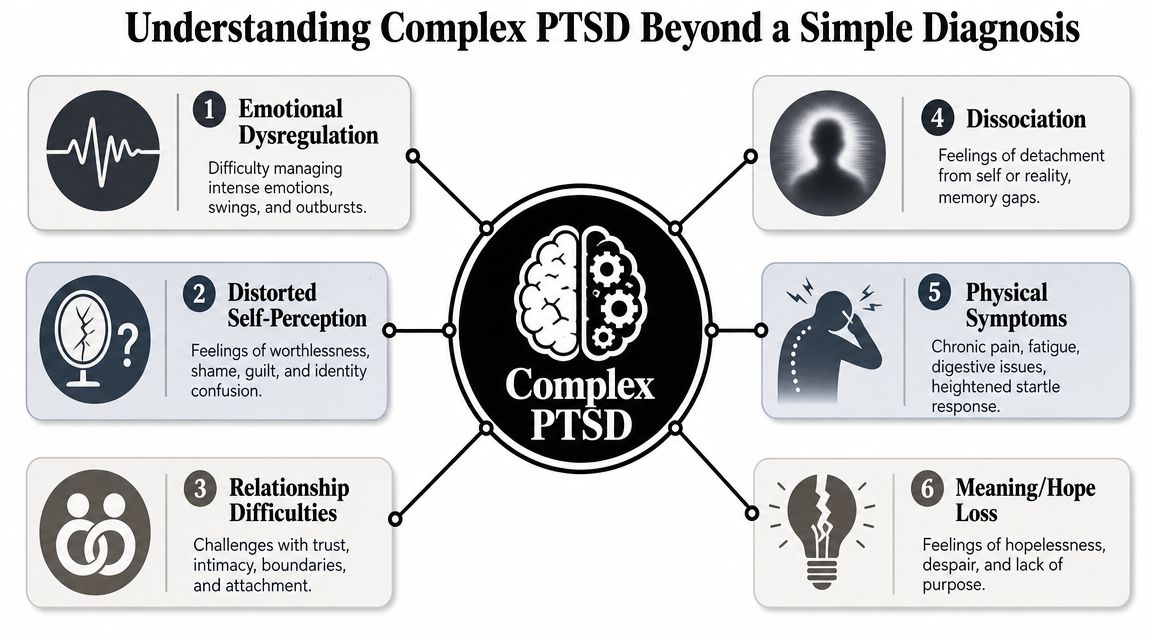
The three patterns attorneys most often notice
The first is affect dysregulation. The client becomes flooded, shuts down, or swings between the two. During testimony preparation, they may go from detailed recall to trembling silence in minutes. That's not necessarily avoidance in the ordinary sense. It may be a nervous system shifting from engagement to survival mode.
The second is a disturbed self-concept. Many survivors don't just remember what was done to them. They organize their identity around blame, contamination, worthlessness, or helplessness. That can distort how they answer even simple questions. A client may minimize extreme abuse because they believe they "deserved" it, or because shame narrows what they can say aloud.
The third is relational disruption. Repeated trauma, especially when caused by caregivers, partners, gangs, traffickers, or officials, alters how a person reads safety. In practice, that can look like mistrust of counsel, dependency on abusive figures, repeated contact with dangerous people, or fear of authority that interferes with medical and legal follow-through.
Additional features that complicate testimony
Complex trauma rarely stays confined to emotion. It often affects attention, bodily reactions, sleep, startle, and memory continuity. A declaration can therefore contain gaps that are clinically unsurprising but legally uncomfortable.
Short examples help:
- Dissociation: the client "goes away" during an interview, loses time, or recalls scenes without sequence.
- Body-based recall: they cannot narrate the event first, but they can describe choking sensations, nausea, shaking, or numbness.
- Meaning collapse: they speak as if the future doesn't exist, which can undermine treatment adherence and case participation.
- Attachment conflict: they fear the abuser and still defend them.
In forensic work, "inconsistent" and "deceptive" are not interchangeable. Complex trauma often disrupts retrieval, sequencing, and emotional access without changing the underlying truth of the abuse history.
What this means for an immigration case
Attorneys can use this framework to interpret behavior that otherwise looks puzzling. The client who misses details may still provide a clinically coherent account. The client who returns to an abusive partner may still meet the legal standard. The client who cannot describe chronology may still clearly convey pattern, coercion, and fear.
A useful analogy is a building with repeated water damage. You don't assess it by looking for one crack in one wall. You look at the structure, the leaks, the warped beams, and the rooms that can no longer be used safely. Complex PTSD works the same way. The forensic question isn't only "Did a traumatic event occur?" It is also "How did repeated trauma alter this person's functioning across settings?"
How EMDR Therapy Reprocesses Traumatic Memories
EMDR makes more sense when you stop thinking of memory as a video file and start thinking of it as a poorly run archive. In uncomplicated memory storage, the mind files an event, links it to context, and recognizes that it is over. In traumatic storage, some material remains loose in the system. A sound, smell, authority figure, locked room, or phrase can pull it back into the present as if the danger is happening now.
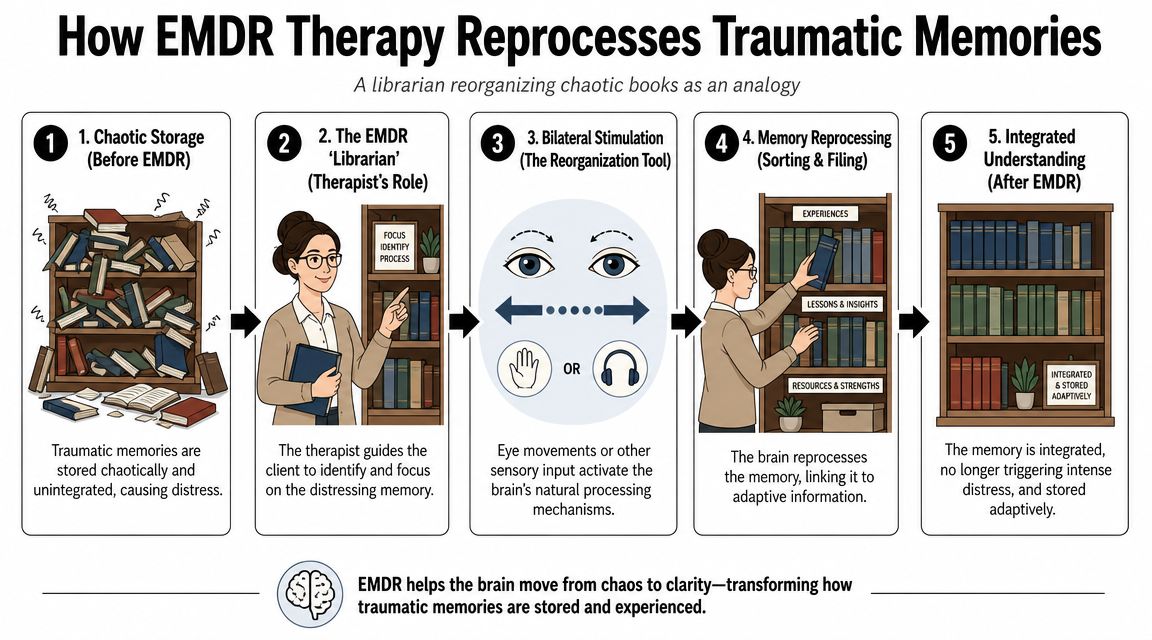
The librarian analogy
Think of the therapist as a librarian helping the client sort a chaotic archive. The therapist doesn't erase the book. The therapist helps the brain identify where it belongs, what it means, and that it is not the only book in the building.
That is why EMDR is often misunderstood. It isn't hypnosis, and it isn't forced disclosure. It is a structured trauma therapy designed to help distressing memories connect with more adaptive information so the memory loses some of its immediate charge. For a concise overview of the therapy's broader applications, attorneys who want a nontechnical primer can review benefits of EMDR in clinical practice.
The eight phases in practical terms
Standard EMDR is typically described in eight phases. For attorneys, the important point is not memorizing labels. It is understanding what each phase contributes to safe and defensible treatment.
History taking
The clinician identifies trauma themes, current symptoms, and readiness. In immigration work, this phase often reveals whether the case involves single-event trauma or layered interpersonal trauma.Preparation
The client learns grounding and stabilization skills. Without this phase, later processing can become destabilizing.Assessment
A specific target is identified, along with the negative belief attached to it and the more adaptive belief the client is working toward.
A short visual can help make the sequence concrete.
Desensitization
The client focuses on the memory while the therapist uses bilateral stimulation, often eye movements, tapping, or alternating tones. The point isn't distraction. The point is to support reprocessing while the memory is activated.Installation
The therapist strengthens the more adaptive cognition connected to the target.Body scan
The client notices whether distress remains in the body. Trauma isn't only verbal; it often persists somatically.Closure
The session ends with grounding. This is especially important when the target is not fully processed in one sitting.Reevaluation
The next session checks what changed, what remains active, and whether the target or plan should shift.
EMDR doesn't ask whether the memory disappears. It asks whether the memory still controls the person's present-tense reactions.
Why this model matters in forensic settings
A clinician who can explain these steps clearly is more likely to produce records that make sense to non-clinicians. That matters when treatment notes or a summary letter must later answer practical questions: Why was this target chosen? Why was processing paused? Why did the therapist spend multiple sessions on preparation? Why did symptoms improve in one domain but not another?
Those questions become even more important when the client has complex trauma, because the standard sequence usually needs significant modification.
Adapting the EMDR Protocol for Complex Trauma Survivors
The biggest mistake in complex PTSD EMDR work is assuming the standard protocol only needs to be slowed down a little. In reality, complex trauma often requires a different rhythm, different targets, and different expectations.
Clinical sources describing EMDR for complex trauma emphasize selective and titrated targeting rather than exhaustive event-by-event processing. They describe the use of representative memories or theme clusters, smaller “chunks,” frequent grounding checks, resource installation such as a safe place or inner protector, and dissociation screening before reprocessing begins (clinical discussion of EMDR adaptations for complex trauma). That approach fits what many forensic clinicians see in immigration-related trauma. The problem usually isn't a shortage of traumatic material. It's too much unintegrated material.
What adapted EMDR changes
With single-incident PTSD, the clinician may choose one index trauma and process it directly. With complex trauma, that can backfire. If the therapist opens a dense cluster of abuse memories too quickly, the client may lose grounding, become highly dysregulated, or stop treatment entirely.
Instead, adapted work often looks like this:
- Longer preparation: more time building grounding, containment, and internal resources
- Theme-based targeting: selecting representative memories linked to a repeated pattern such as humiliation, captivity, or betrayal
- Chunking: processing manageable slices of memory rather than the entire trauma chain
- Frequent state checks: monitoring whether the client is still present, oriented, and able to regulate
- Flexible closure: ending with stabilization, even when full processing must wait
Standard EMDR vs adapted EMDR for Complex PTSD
| Phase/Aspect | Standard EMDR (Single-Incident PTSD) | Adapted EMDR (Complex PTSD) |
|---|---|---|
| Primary target | One clearly identified event | Representative memory, theme cluster, or smaller fragment |
| Preparation | Briefer if the client is stable | Often extended to build grounding and internal safety |
| Pacing | More direct access to target memory | Titrated processing with frequent pauses and checks |
| Memory structure | More coherent event sequence | Fragmented, sensory, shame-based, or body-driven material |
| Dissociation focus | Important but may be less central | Screening is essential before and during reprocessing |
| Goal of early treatment | Reduce distress linked to one event | Increase stability while processing trauma without flooding |
| Therapist stance | Standard protocol sequence | Highly flexible within a phased trauma framework |
What works and what doesn't
What works is precision. The therapist picks the right target, the right dose of activation, and the right time to stop. This parallels adjusting light in a darkroom. Too little exposure, and the image doesn't develop. Too much, and the image burns out.
What doesn't work is exhaustive storytelling under the banner of processing. A client doesn't need to relive every assault, detention episode, or trafficking act in sequence for EMDR to be clinically meaningful. In fact, trying to process everything at once can make the work less safe and less effective.
Clinical caution: In complex trauma, more memory activation is not always better treatment. Good EMDR often looks measured, repetitive, and slower than the client or attorney expected.
For attorneys, this distinction can guide referrals. Ask whether the clinician works with dissociation, how they choose targets in prolonged trauma, and what they do if the client becomes overwhelmed. If the answer sounds rigid or overly optimistic, that is useful information.
Reviewing the Evidence and Managing Outcome Expectations
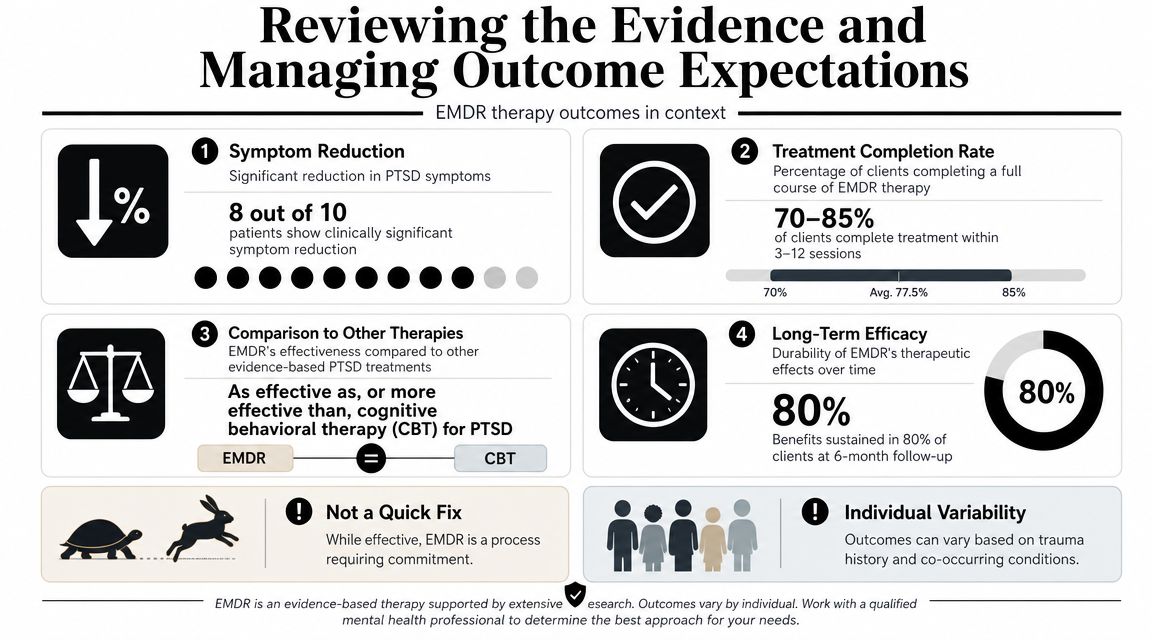
EMDR has a substantial research base for PTSD, and attorneys should know the evidence well enough to avoid two opposite mistakes. One is dismissing EMDR as trendy. The other is treating it as a guaranteed cure for every complex trauma presentation.
A major review in the Journal of Traumatic Stress reported that across published randomized controlled trials, remission rates ranged from 36% to over 90%; in one study, nearly 70% of participants no longer met PTSD diagnostic criteria after treatment, and at 1-year follow-up more than 80% no longer met diagnostic criteria. The same review noted that EMDR remained highly effective at reducing posttraumatic stress, depressive, and anxiety symptoms, with gains maintained at 6 months in some studies (Journal of Traumatic Stress review of EMDR outcomes).
How to read those numbers responsibly
Those findings matter because they show EMDR is a serious, evidence-based trauma treatment. But they do not mean every immigration client with complex trauma will move through therapy on a standard timeline or achieve full symptom resolution.
Research on PTSD often supplies the evidentiary anchor for complex trauma treatment, yet complex cases usually involve added burdens: dissociation, chronic shame, interpersonal betrayal, fragmented recall, unstable housing, ongoing legal stress, and current safety threats. Those factors don't negate EMDR. They change how progress should be judged.
Better outcome benchmarks for attorneys
In a legal context, the most useful treatment benchmarks are often functional rather than dramatic. Look for signs such as:
- Greater interview tolerance: the client can discuss core events with less shutdown or disorganization
- Improved daily functioning: sleep, concentration, parenting, or work capacity becomes more stable
- Reduced body panic: fewer intense physiological reactions when trauma cues arise
- More coherent thematic narrative: not perfect chronology, but clearer links between abuse and current symptoms
A good analogy is physical rehabilitation after multiple fractures. The measure of success isn't only whether the pain vanished. It is whether the person can stand longer, move more safely, and use the injured limb with less fear.
Expect a non-linear course
Complex trauma treatment often proceeds unevenly. Some sessions produce obvious relief. Others stir up grief, anger, or somatic distress before the client regains equilibrium. Attorneys should be careful not to interpret temporary increases in distress as proof that treatment is failing.
What matters is whether the clinician can explain the trajectory in a disciplined way. A credible treatment summary distinguishes between temporary activation, meaningful symptom change, unresolved domains, and ongoing need for care. That kind of realism usually strengthens, rather than weakens, the evidentiary value of the record.
Essential Safety Protocols and When to Postpone EMDR
A trauma treatment plan isn't sound just because it includes EMDR. In complex cases, safety depends on timing, preparation, and the clinician's willingness to postpone reprocessing when the client is not ready.
Patient-facing material often says EMDR can help CPTSD, but it rarely answers the difficult question attorneys ask in practice: when should treatment pause rather than proceed? Clinical guidance notes that EMDR is often modified for longer-term trauma with added preparatory work such as grounding, containment, affect regulation, and dissociation screening, and that more complex or longer-term trauma may require 8–12 sessions or more rather than the 3–6 sessions often cited for a single event. The same clinical discussion notes a recent case report suggesting EMDR may work better for CPTSD when combined with schema therapy and imagery rescripting (Cleveland Clinic overview of EMDR therapy and complex presentations). That is a useful corrective to one-size-fits-all messaging.
Red flags that call for delay or extra caution
Some clients need more stabilization before direct trauma processing. Others need a blended treatment plan rather than EMDR alone.
Key warning signs include:
- Active dissociation: the client loses time, depersonalizes, or repeatedly disconnects during emotionally loaded discussion
- Current danger: ongoing domestic violence, trafficker control, stalking, or unstable housing
- Severe self-harm or suicidality concerns: trauma activation may exceed the client's ability to recover between sessions
- Extremely weak grounding skills: the client cannot reliably return to the present after activation
- Overwhelming legal stress: a major filing, hearing, or detention event may make intensive reprocessing poorly timed
Attorneys who need a broader framework for evaluating readiness can also review a trauma-informed care assessment approach for legal and clinical settings.
What a safe stabilization phase includes
A proper stabilization phase isn't "doing nothing." It is active treatment. The clinician may teach orientation exercises, containment imagery, paced breathing, sensory grounding, body awareness, or ways to identify early signs of dissociation. The client may also learn how to stop processing, ask for breaks, and track post-session destabilization.
A client who can say, "I'm starting to disappear," is often safer than a client who says, "I'm fine," while visibly shutting down.
This phase can frustrate attorneys who want rapid symptom relief before an affidavit or hearing. But rushing can create worse problems. If the client becomes destabilized, they may miss appointments, avoid legal preparation, or become less able to provide a coherent history.
When combination treatment makes more sense
Not every complex trauma case should rely on EMDR alone. Some people need parallel work on entrenched shame, relational patterns, or self-attack before or alongside reprocessing. That doesn't dilute EMDR. It reflects good case formulation.
In forensic terms, a prudent clinician should be able to explain why they chose EMDR now, why they postponed it, or why they combined it with other modalities. That explanation often matters as much as the treatment label itself.
Translating EMDR Treatment into Persuasive Legal Evidence
Good therapy can still produce weak evidence.
In immigration cases, the problem is rarely that EMDR occurred. The problem is that the record often fails to show what the clinician observed, why the treatment was paced a certain way, and how those observations relate to credibility, functioning, and risk. USCIS officers and immigration judges do not need marketing language about trauma treatment. They need a clear chain of reasoning they can follow.
For attorneys, this distinction matters. A treatment note saying the client "processed trauma" does little work in an asylum, VAWA, T visa, U visa, or hardship case. A note explaining that treatment targeted confinement cues tied to detention, that the client showed panic and derealization when discussing closed spaces, and that symptom intensity decreased only after careful phased work is far more useful. That is evidence. It shows method, observation, and limits.
What attorneys should want in the record
A persuasive treatment summary answers forensic questions. It does not read like a billing note or a self-congratulatory discharge summary.
The record should document:
- Why EMDR was used, delayed, or combined with another approach. That choice tells the court whether the clinician exercised judgment or applied a standard protocol.
- How the trauma was organized for treatment. In complex PTSD, targets are often clustered around repeated themes such as captivity, coercive control, betrayal, sexual humiliation, or forced dependency.
- What risks affected pacing. Dissociation, fragmented recall, panic, self-blame, unstable housing, ongoing abuse, and fear of authorities all affect how much reprocessing is clinically safe.
- What the clinician did. Preparation work, target selection, grounding methods, shortened sets, interruptions, and return-to-stability procedures should appear in the record.
- What changed over time. The strongest descriptions are concrete: fewer panic symptoms during legal preparation, better ability to discuss key events, reduced physiological reactivity, improved sleep, or less avoidance of attorney contact.
- What remained impaired. Courts should see the continuing limits, not just gains. Persistent shame, dissociation, nightmares, startle, memory gaps, and relational fear often remain even when treatment helps.
That last point is often mishandled. Improvement does not mean the trauma effects were minor. In forensic work, partial improvement can strengthen the record because it shows the clinician tracked change carefully instead of overstating outcome.
What good forensic wording sounds like
Clinical precision matters more than enthusiasm.
"Client reported reduced panic when discussing detention-related confinement after phased EMDR work focused on representative confinement triggers" is useful. "EMDR resolved detention trauma" is not. The first statement ties intervention to an observed shift. The second invites cross-examination because it overclaims.
The same rule applies to memory. A careful clinician might write, "Treatment addressed recurring themes of coercion, humiliation, and threat associated with repeated partner abuse. Client's recall remained uneven, but discussion became more organized and less physiologically overwhelming across sessions." That wording helps an attorney explain why the client may present with fragmented but clinically consistent recall.
Some cases require more than treatment notes and a diagnosis. Where attention, memory, concentration, or executive functioning are disputed, attorneys may also need a detailed neuropsychological evaluation framework to separate trauma-related impairment from malingering claims, developmental issues, head injury, or severe depression.
How to connect treatment to the legal narrative
The clinician should not become a fact witness for every alleged event. That is poor forensic practice and poor risk management. The better approach is to document trauma patterns, current symptoms, treatment decisions, and observed response, then let the attorney fit that material into the legal theory of the case.
I advise attorneys to look for a structure like this:
Identify the trauma pattern
Prolonged domestic violence, trafficking-related coercion, detention abuse, chronic childhood maltreatment, or repeated assault by authority figures.Describe the present clinical effect
Panic during interviews, shutdown when asked for dates, shame-based minimization, dissociative detachment, nightmares, avoidance, or difficulty sustaining a linear narrative.Explain how EMDR was adapted
Theme-based target selection, smaller pieces of processing, extended preparation, frequent grounding, and pauses when activation rose too quickly.State the result conservatively
Better affect regulation, greater tolerance for discussing traumatic material, less somatic reactivity, or improved ability to work with counsel.
That structure works like chain of custody for psychological evidence. If one link is missing, the opinion becomes easier to attack. If the clinician can show what was observed, why a treatment choice was made, and what changed afterward, the record becomes harder to dismiss as generic therapy language.
For immigration attorneys, the practical payoff is straightforward. Strong EMDR documentation can explain delayed disclosure without excusing every inconsistency. It can show why fragmented memory is clinically expected in complex trauma. It can support hardship and credibility arguments by tying symptoms to observed impairment rather than broad diagnostic labels. It can also show that the treating clinician acted cautiously, which matters when opposing counsel argues that the record is advocacy disguised as treatment.
If you need immigration-focused psychological evidence that connects trauma history, diagnosis, and treatment considerations in a legally usable format, Pro Psychological Analysis provides forensic evaluations for asylum, VAWA, T visa, U visa, and hardship cases. The practice works with attorneys to document trauma with clinical rigor, clear methodology, and careful attention to admissibility, confidentiality, and case deadlines.