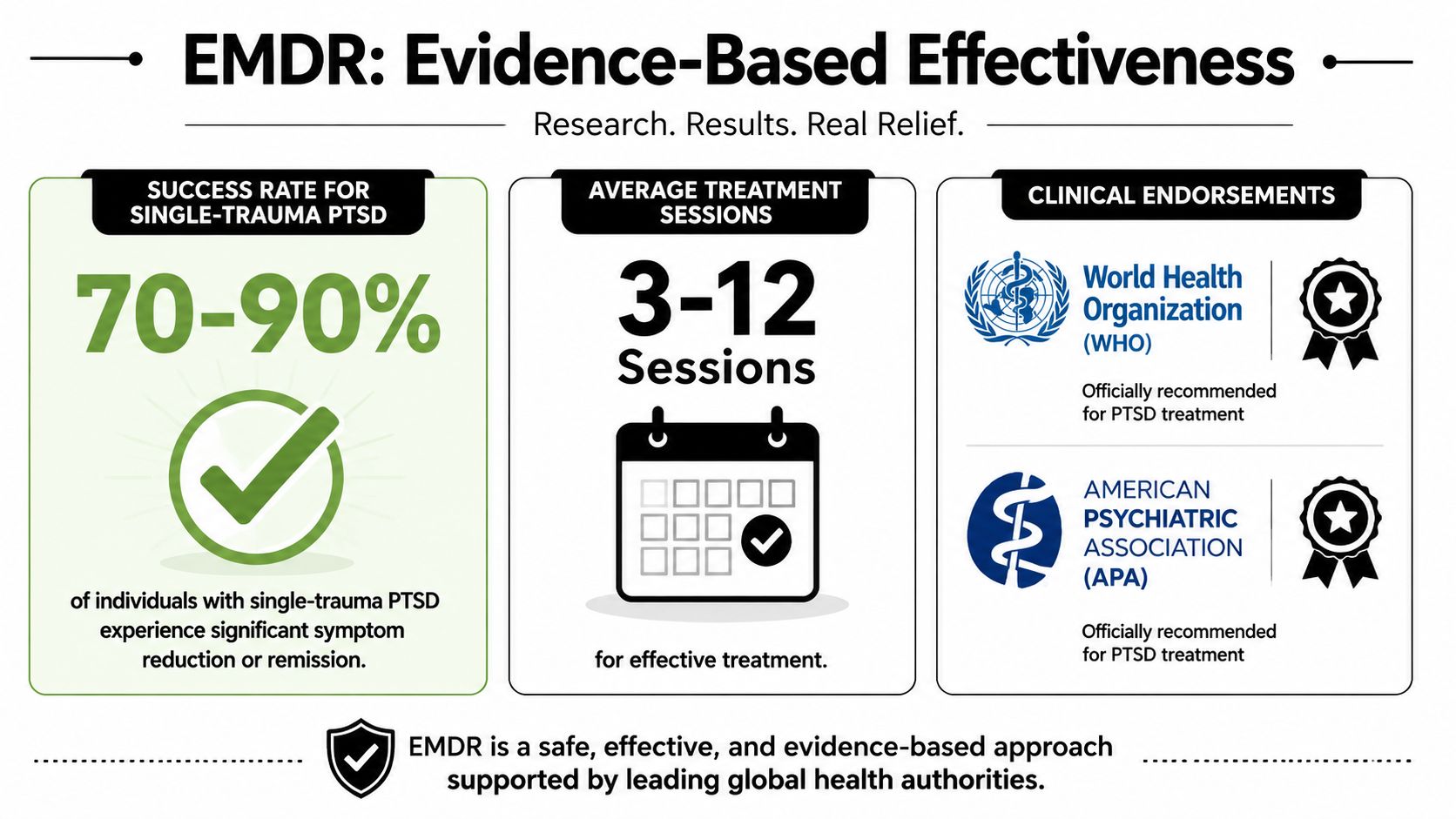
EMDR is an eight-phase psychotherapy that uses bilateral stimulation to help the brain reprocess traumatic memories, and it is one of the most evidence-based treatments for PTSD and related trauma conditions. In single-trauma cases, 84% to 90% of people no longer meet PTSD criteria after three 90-minute sessions, and EMDR is recognized as a first-line treatment by the WHO and APA.
If you're an immigration attorney, you may be dealing with a client who can't tell their story in a straight line, shuts down when asked about abuse, or looks inconsistent on paper even though the trauma is real. If you're the client, you may know exactly what happened but still feel unable to describe it without panic, shame, numbness, or confusion.
That gap matters in legal work. Immigration cases often turn on credibility, symptom severity, functional impairment, and a clear connection between trauma and current hardship. Trauma can interfere with all of that. A client may remember events in fragments, avoid key details, or minimize what happened because recounting it feels unbearable.
EMDR matters here because it isn't just a therapy buzzword. It's a structured clinical method with a defined protocol, strong research support, and a practical role in cases involving asylum, VAWA, T visas, U visas, and extreme hardship waivers. In the right setting, it can help reduce symptom intensity while also clarifying the psychological impact of trauma in a way that becomes useful for forensic documentation.
For attorneys, the key question usually isn't whether EMDR sounds groundbreaking. It's whether it produces clinically reliable information that can support a legal claim. Sometimes it does. Sometimes it doesn't, especially when the clinician lacks forensic judgment or the case calls for assessment before treatment.
The useful way to approach EMDR is not as magic and not as a replacement for a forensic evaluation. It's a tool. Used well, it can help a traumatized person process specific memories, reduce reactivity, and describe their experience with more stability. Used poorly, it can blur treatment goals and legal goals.
Table of Contents
- Introduction A Path Through Trauma
- The Core Theory Behind EMDR How It Reprocesses Trauma
- The 8 Phases of EMDR A Step-by-Step Treatment Journey
- The Evidence for EMDR Success Rates and Clinical Endorsements
- Using EMDR Findings in Immigration and Forensic Evaluations
- Practical Guidance for Attorneys and Clients
- Frequently Asked Questions About EMDR Treatment
Introduction A Path Through Trauma
In immigration practice, trauma rarely arrives in neat chronology. A client may start with the arrest, skip the assault, minimize the domestic violence, and only later mention detention, threats, or coercive control. That doesn't mean the account is false. It often means the nervous system is still organized around survival rather than storytelling.
For legal decision-makers, that distinction is critical. Adjudicators and courts look for consistency, functional impact, and clinical support. Yet trauma often produces avoidance, fragmentation, shame, emotional numbing, and abrupt shifts in memory access. A person can be truthful and still struggle to narrate events coherently.
Practical rule: When a client can't speak linearly about trauma, don't assume resistance or exaggeration. First consider whether trauma itself is disrupting recall, affect regulation, and disclosure.
The question "What is EMDR treatment?" takes on greater importance than general mental health education. In practice, EMDR is a structured psychotherapy that can help trauma survivors process disturbing memories without requiring prolonged verbal retelling. For some clients, that makes the difference between shutting down and being able to participate meaningfully in treatment.
EMDR also has a second relevance in immigration work. It can generate clinically useful observations about triggers, negative beliefs, body-based distress, and functional impairment. Those aren't legal conclusions, but they often become important pieces of a psychological evaluation when the clinician knows how to translate them into forensic language.
Why this matters in legal settings
Attorneys usually need answers to practical questions:
- Can the client tolerate discussing the traumatic material: Some clients can't manage traditional talk therapy early in treatment.
- Will treatment clarify or confuse the timeline: The answer depends heavily on timing, documentation, and the clinician's methods.
- Does the intervention address only PTSD: No. EMDR is also being used in trauma-related presentations that don't fit classic single-event PTSD.
- Can treatment observations support an evaluation: Yes, but only when the clinician separates treatment from forensic opinion and documents carefully.
A good EMDR clinician doesn't promise to produce the perfect declaration. That's not how ethical work looks. Its fundamental value is more disciplined. EMDR can reduce the emotional intensity of traumatic memories, improve regulation, and help clients engage with their legal case without becoming overwhelmed.
Trauma treatment and forensic evaluation serve different functions. The strongest legal work happens when both are coordinated, but not confused.
The Core Theory Behind EMDR How It Reprocesses Trauma
A client sits in an attorney's office and tries to answer a simple timeline question about detention, assault, or coercive control. The facts are there, but the body reacts first. Breathing changes. Attention narrows. Shame, fear, or numbness takes over. In clinical terms, that response suggests the memory is still stored in a maladaptive form, with its original sensory, emotional, and belief-based charge intact.
EMDR is built on the Adaptive Information Processing model, or AIP. The model holds that under normal conditions, the brain integrates experience and stores it in a way that allows recall without full re-experiencing. Trauma can disrupt that process. The memory remains accessible, but it is linked too tightly to the original distress, body sensations, and negative meanings.
A legal file comparison is useful here. A damaged record can still exist in the system, yet every attempt to open it triggers errors, mislabeling, or missing context. Traumatic memory can function in a similar way. A smell, date, interview room, government letter, or interpersonal conflict can activate a network that feels present rather than past.
How the AIP model explains trauma symptoms
The person does not merely "think about" what happened; they may re-enter the emotional and physiological state tied to the event. This can look like panic, shutdown, dissociation, irritability, somatic distress, guilt, or fixed beliefs such as "I am unsafe," "I deserved this," or "I failed to protect my child."
Those beliefs are often clinically relevant in immigration work. Asylum cases may involve chronic fear and helplessness after persecution. VAWA cases may involve coercive control, shame, and attachment-based trauma. Hardship cases may involve prolonged anxiety, moral injury, and persistent anticipatory dread related to family separation, medical risk, or forced return. EMDR is often associated with PTSD, but the underlying treatment logic applies more broadly to trauma-linked memory networks that continue to drive present functioning.
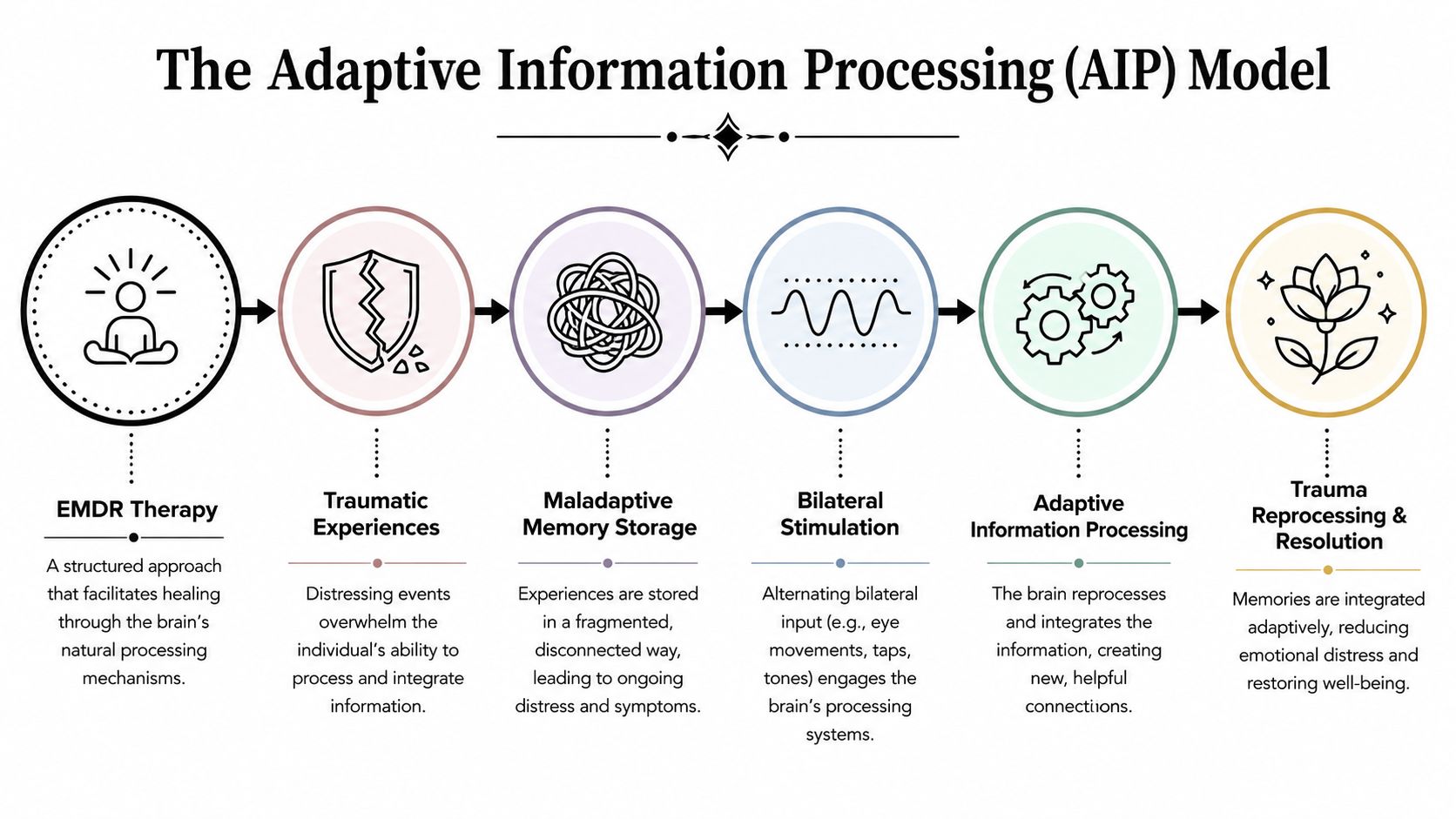
The treatment goal is precise. EMDR aims to help the brain link the traumatic memory with more adaptive information, so the person can recognize, "This happened in the past. It is not happening now." The event is not erased. The historical facts remain the same. What changes is the level of activation and the meaning attached to the memory.
That distinction has forensic value. In a sound evaluation, reduced flooding can improve a client's ability to recount events with greater tolerance, more continuity, and less collapse under questioning.
The Role of Bilateral Stimulation in Sessions
Bilateral stimulation, or BLS, usually involves side-to-side eye movements, alternating taps, or alternating tones. During processing, the client holds a target memory in mind in a controlled way, including the image, negative belief, emotion, and body sensation associated with it. The therapist then uses BLS in brief sets while monitoring distress, attention, and stability.
The mechanism is still debated in the literature, but the clinical pattern is familiar. With proper preparation and pacing, many clients report that the memory becomes less vivid, less physically overwhelming, and less fused with beliefs such as "I am powerless" or "the danger is still here." New associations often appear. A client may connect the event to a larger context, recognize survival responses more accurately, or shift from self-blame to a more reality-based interpretation.
The process is structured and disciplined. Clients do not need to provide a long, continuous narrative in every set. That can be useful in cases where detailed verbal retelling would predictably push the person outside their window of tolerance.
Several trade-offs matter in practice:
- EMDR preserves memory while reducing reliving: clients usually continue to remember the event, but with less physiological intensity.
- Pacing determines whether processing is helpful or destabilizing: clients with severe dissociation, acute instability, or major external stressors may need more preparation before trauma targets are addressed.
- Clinical gains do not automatically equal forensic conclusions: symptom change, triggers, body responses, and negative cognitions can inform an evaluation, but they still require careful interpretation in the legal context.
The clinical aim is to convert a memory from a present-tense threat response into a past-tense narrative the client can access without being overtaken by it.
For immigration attorneys, that is the practical point. EMDR can improve emotional regulation and access to difficult material. In some cases, it also clarifies patterns that matter in forensic assessment, including avoidance, fragmented recall under stress, moral injury after forced acts or failed protection, and prolonged anxiety tied to removal, persecution, or family separation.
The 8 Phases of EMDR A Step-by-Step Treatment Journey
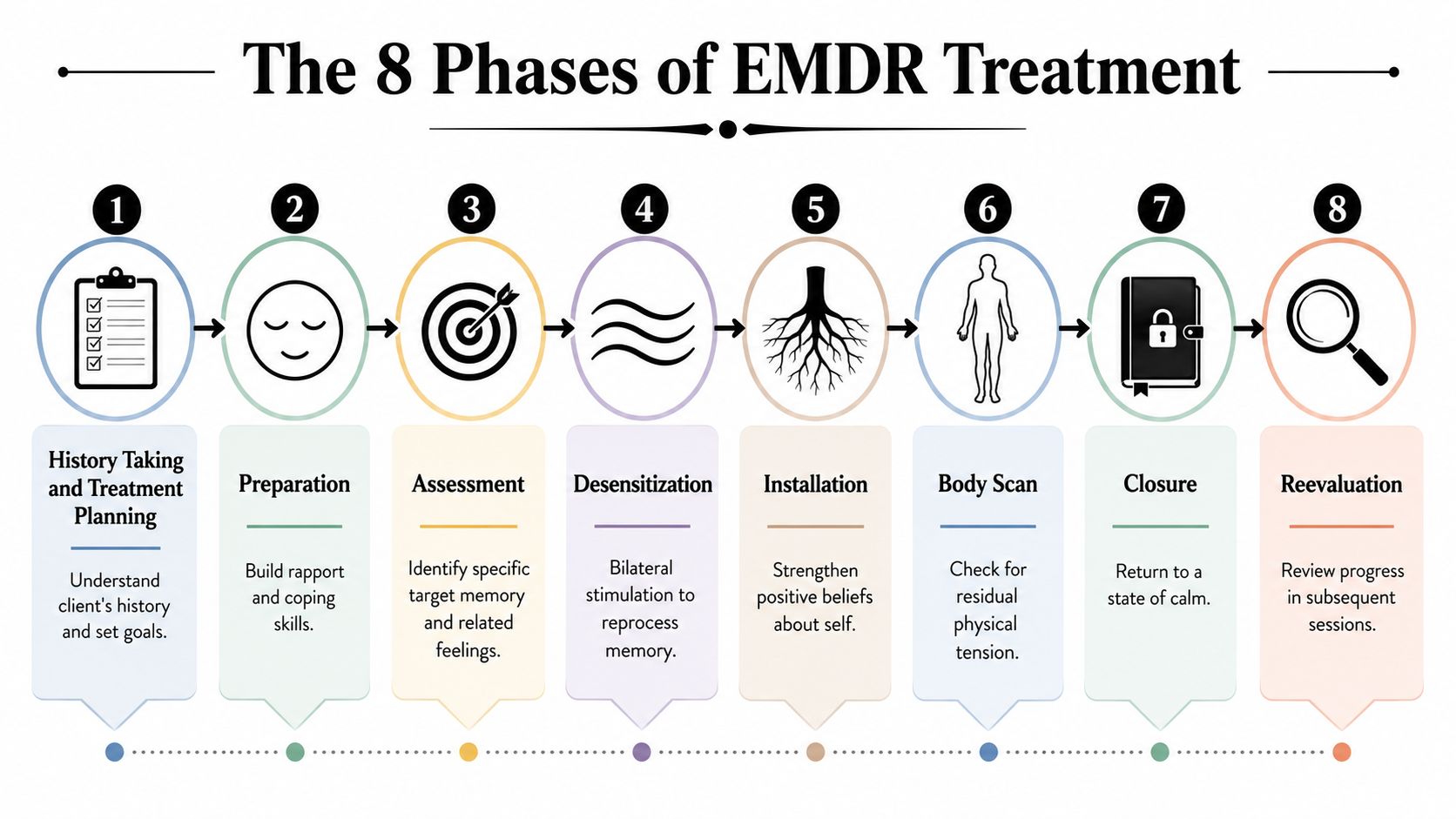
EMDR has an eight-phase treatment model. That matters because many clients and referring attorneys assume EMDR is just eye movements while talking about trauma. It isn't. The eye movements are only one part of a larger protocol designed to assess readiness, target the right memories, process them systematically, and check whether the change holds.
Phases 1 through 3 building safety and selecting the target
Phase 1 is history taking and treatment planning. The clinician gathers the client's background, identifies presenting symptoms, and decides what memories or experiences may become treatment targets. In forensic-adjacent situations, this is also where timing matters. If an immigration filing is imminent, the clinician should think carefully about whether active trauma processing is clinically appropriate before declarations, affidavits, or testimony preparation.
Phase 2 is preparation. This phase is often underestimated. The therapist explains EMDR, builds rapport, and teaches regulation skills so the client can tolerate distress without becoming overwhelmed. If a client has severe dissociation, unstable functioning, or poor grounding capacity, this phase may take longer than people expect.
Phase 3 is assessment. The clinician and client identify a specific target memory and map its parts. That usually includes the image that best represents the memory, the negative belief attached to it, the preferred positive belief, emotions, and body sensations. This precision is one reason EMDR can be useful in legal contexts. It links symptoms to concrete experiences rather than leaving the trauma history vague.
A simple summary looks like this:
| Phase | What happens | Why it matters |
|---|---|---|
| 1 History | Clinical history and target selection | Prevents unfocused treatment |
| 2 Preparation | Stabilization and coping skills | Reduces risk of overwhelm |
| 3 Assessment | Defines the target memory and associated beliefs | Creates a clear treatment focus |
Phases 4 through 6 active reprocessing and belief change
Phase 4 is desensitization. This is the part often associated with EMDR. The client holds the target in mind while following bilateral stimulation. After each set, the therapist checks what the client noticed and continues based on the emerging material. The work is active, but it should still feel contained.
Phase 5 is installation. Once the distress linked to the target drops, the clinician strengthens the preferred positive belief. If the original belief was "I am powerless," the newer belief may be closer to "I survived" or "I have choices now." The therapist isn't coaching false positivity. The goal is a belief that feels emotionally credible.
Phase 6 is the body scan. Trauma often persists in somatic form even after the narrative feels less disturbing. The client notices whether any tension, pain, pressure, or unease remains while thinking of the target and new belief. If the body is still reacting, more processing may be needed.
Good EMDR isn't only about what the client says. It's also about whether the body still registers unresolved threat.
These middle phases are where clinicians can either do careful work or create problems. Poor pacing, unclear target selection, or inadequate stabilization can leave the client flooded rather than helped. That's why an attorney shouldn't treat "offers EMDR" as enough of a credential by itself.
Phases 7 and 8 ending well and checking the work
Phase 7 is closure. Every session should end with the client back in a manageable state, even if processing isn't complete. Closure may involve grounding, orienting to the present, or using calming techniques rehearsed earlier.
Phase 8 is reevaluation. At the next session, the therapist checks whether the gains held, whether distress returned, and whether the target is resolved. If not, work continues. If so, the clinician may move to related memories, current triggers, or future situations.
For attorneys and clients, the practical lesson is that EMDR should feel structured. A competent provider can explain where the client is in the sequence, what target is being addressed, and why the timing makes sense. If the process feels improvised from one session to the next, that usually signals a clinical problem.
The Evidence for EMDR Success Rates and Clinical Endorsements
An attorney preparing an asylum or VAWA case may ask a simple question: is EMDR a credible treatment, or will it look experimental on review? In clinical practice and in forensic settings, EMDR is established, widely studied, and accepted by major professional bodies. That matters because a treatment method carries more weight in a legal record when it rests on recognized standards rather than therapist preference.
What the outcome literature supports
The strongest support for EMDR comes from controlled trauma research and from formal treatment guidelines, not from marketing summaries. The EMDR International Association summary of research describes multiple randomized studies showing benefit for trauma symptoms, particularly PTSD. The World Health Organization guidelines on conditions related to stress include EMDR among recommended trauma-focused interventions, and the U.S. Department of Veterans Affairs PTSD guidance recognizes it as an evidence-based treatment.
That level of endorsement is clinically meaningful.
It does not mean EMDR works the same way for every client, every diagnosis, or every trauma history. Single-incident trauma often responds faster than chronic interpersonal violence, trafficking-related coercion, prolonged detention trauma, or the layered fear found in many immigration cases. In those cases, the treatment target is often broader than a classic PTSD memory. The clinician may also need to address shame, moral injury, persistent threat, and prolonged anxiety that continue even after the client is physically safe.
For attorneys and clinicians who want a treatment-focused overview, these benefits of EMDR in clinical practice are useful background.
A more conservative reading of the evidence is the right one for legal work. EMDR has solid support as a first-line trauma treatment. It also has limits. The published literature is strongest for PTSD and trauma-related symptoms, while immigration evaluations often involve mixed presentations that include depression, dissociation, grief, somatic distress, and fear tied to unstable legal status or family separation. A competent evaluator does not stretch the research beyond what it supports.
How clinical endorsement translates to forensic value
In forensic immigration evaluations, endorsement serves two functions. First, it shows that the treating method is mainstream and recognizable to courts, agencies, and opposing reviewers. Second, it helps the evaluator explain why symptom change, trauma triggers, or persistent impairment were assessed through a method with accepted clinical standing.
That does not convert treatment into proof of a legal claim. It strengthens the reliability of the clinical narrative.
There is also a practical trade-off. Effective EMDR can reduce visible distress before the evaluation is completed. A client who previously had panic, fragmented recall, insomnia, or intense autonomic reactivity may present as calmer after treatment begins. In a weak report, that improvement can be misread as evidence that the original trauma impact was minor. In a careful report, the evaluator documents baseline symptoms, course of treatment, response over time, and what remains impaired despite improvement.
Some clients are also poor candidates for immediate trauma processing. Severe dissociation, active psychosis, unstable substance use, or inability to maintain present orientation can require stabilization first. That point matters in legal cases because a delay in EMDR is not evidence of exaggeration or treatment resistance. It may reflect sound clinical judgment.
For asylum, VAWA, and hardship matters, that distinction is more than academic. A credible evaluation often depends on showing not only that trauma occurred, but how the person's symptoms developed, why they persisted, and whether treatment response is consistent with the claimed history. EMDR fits that framework well when it is used carefully and documented with forensic discipline.
Using EMDR Findings in Immigration and Forensic Evaluations
In immigration work, the most important question isn't whether EMDR helps trauma. It's whether EMDR-related findings can support a legally relevant psychological narrative without overstepping the line between treatment and forensic opinion.
The answer is yes, when the work is done carefully. In asylum, VAWA, T visa, U visa, and hardship matters, trauma often affects memory organization, fear response, self-blame, trust, sleep, concentration, and daily functioning. EMDR can help identify which experiences remain psychologically active and how those experiences connect to present impairment.
Where EMDR fits in asylum VAWA and hardship work
A treatment-informed evaluation may document patterns such as these:
- Trigger-linked distress: The client becomes reactive when discussing detention, partner violence, extortion, trafficking, or family separation.
- Negative self-beliefs: Themes like shame, helplessness, contamination, or unworthiness appear consistently around target memories.
- Somatic activation: Body-based fear responses emerge even when the client gives only minimal verbal detail.
- Functional impairment: Avoidance, panic, sleep disruption, emotional numbing, and concentration problems interfere with work, caregiving, or legal participation.
Those findings can be highly relevant in a forensic report. They don't prove the underlying events by themselves, but they can support the clinical plausibility of the account and explain why a survivor's presentation may look fragmented or inconsistent.
A related issue is timing. Sometimes a full forensic evaluation should occur before trauma processing begins, especially if the legal team needs an undisturbed baseline record of symptoms. In other cases, the client is too dysregulated to participate effectively in any evaluation until some treatment occurs. There isn't a one-size-fits-all answer.
The legal value of EMDR doesn't come from saying "the client had therapy." It comes from documenting symptom patterns, trauma-linked responses, and clinically coherent change over time.
For legal teams dealing with layered trauma histories, this discussion of complex PTSD and EMDR in immigration-related contexts can help frame referral decisions.
Why moral injury and prolonged anxiety matter legally
One of the most important developments in this area is that EMDR is increasingly relevant beyond classic PTSD. Recent clinical trends reported in this discussion of EMDR and its phases describe rising efficacy for non-PTSD complex trauma common in immigration cases, including prolonged anxiety and moral injury, and connect those conditions to USCIS standards in Extreme Hardship and VAWA contexts.
That matters because many immigrant clients were not harmed by one discrete event. They lived through chronic threat. They endured prolonged detention, coercive dependence, repeated discrimination, forced silence, bureaucratic uncertainty, family separation, or repeated exposure to danger. Clinically, those experiences may produce persistent fear, guilt, betrayal, humiliation, and moral conflict without fitting the cleanest PTSD stereotype.
Later in the process, it often helps to give clients and attorneys a brief visual explanation of how trauma treatment can intersect with legal documentation:
In forensic terms, moral injury may appear as profound shame, self-condemnation, betrayal-based distress, or psychological conflict tied to impossible choices. Prolonged anxiety may present as continuous hypervigilance, anticipatory fear, sleep disruption, and impaired concentration driven by chronic legal and social instability. EMDR can help organize and reduce these symptom networks, which in turn can make the resulting evaluation more clinically precise and more legible to adjudicators.
Practical Guidance for Attorneys and Clients
A common referral problem looks like this. Counsel sends a traumatized client to a well-meaning EMDR therapist, treatment starts immediately, symptoms intensify for two weeks, and the client has a declaration interview pending. The issue is rarely EMDR itself. The issue is timing, case coordination, and whether the clinician understands the difference between therapeutic progress and forensic usefulness.
For immigration matters, provider selection is a case strategy question, not just a mental health question. An EMDR clinician may be skilled with standard trauma treatment and still miss problems that matter in asylum, VAWA, or hardship cases, such as inconsistent functioning across settings, moral injury tied to coercive choices, or prolonged anxiety linked to family separation and legal uncertainty.
Questions attorneys should ask before referring
Ask direct questions and listen for concrete answers.
- What EMDR training have you completed: Formal EMDR training matters. So does experience using the protocol with dissociation, chronic trauma, and clients under active legal stress.
- What kinds of trauma cases do you treat most often: Immigration clients often present with cumulative harm, not one isolated event. The clinician should be comfortable with coercive control, detention-related fear, betrayal, shame, and chronic threat.
- How do you document symptoms, functional impairment, and treatment response: Good answers include regular note structure, clear target identification, and careful descriptions of change over time.
- Do you provide therapy, forensic opinions, or both: Those roles require different methods and different boundaries. If one clinician does both, attorneys should clarify how neutrality, informed consent, and record use will be handled.
- How do you manage treatment when declarations, affidavits, or testimony are still pending: This question matters. Memory processing can shift emotional intensity, narrative organization, and avoidance patterns, all of which may affect how a client presents in legal interviews.
If the answers are vague, the referral risk goes up.
What clients should look for in an EMDR provider
Clients should look for a therapist who explains the process clearly and respects the pace required by the case. Early sessions should cover preparation, grounding, and what will happen if distress rises too quickly in session or between sessions.
The provider should also explain why a particular memory, belief, or body sensation is being targeted. In legal cases, that level of clarity helps avoid a common misunderstanding. Treatment is meant to reduce symptom burden and improve functioning. It is not a method for producing a stronger story.
A good clinician also keeps boundaries clear. The therapist is not acting as attorney, case manager, or fact witness unless that role has been explicitly defined and is professionally appropriate. That distinction protects both treatment and the legal record.
- Safety and pacing: The therapist should explain how sessions start, pause, and stop, and how stabilization is handled before trauma processing begins.
- Clear treatment targets: You should know what the clinician is working on and why it was selected.
- Awareness of legal timing: Immigration deadlines, interviews, and court dates can affect whether intensive trauma processing should start now or later.
- Careful records and role clarity: Pro Psychological Analysis provides specialized immigration psychological evaluations focused on trauma documentation and legal relevance. That work is different from ongoing therapy, but in some cases the distinction and coordination plan should be discussed early.
The practical standard is simple. Refer to clinicians who understand trauma, documentation, and professional boundaries. In immigration cases, good EMDR treatment should reduce suffering while preserving the clarity and reliability that legal decision-makers need.
Frequently Asked Questions About EMDR Treatment
Do I have to describe the trauma in detail
Usually, no.
EMDR can be useful for clients who shut down, dissociate, or become flooded when asked to give a long verbal account. The therapist still needs enough information to identify the target memory, the related belief, and the present trigger, but treatment does not depend on a detailed retelling of every event.
That difference matters in immigration cases. A client may be able to engage in trauma treatment without repeating facts in a way that feels exposing or destabilizing, which can be especially relevant in asylum, VAWA, and hardship matters involving sexual violence, coercive control, torture, or detention-related trauma.
Is EMDR hypnosis
No. EMDR is a structured trauma treatment in which the client stays oriented, aware, and able to stop at any point. The therapist directs attention and monitors the client's response, but the client remains in control throughout the session.
For attorneys, the practical issue is memory integrity. Proper EMDR treatment is designed to reduce distress linked to existing memories, not to generate new facts, shape testimony, or coach a narrative. In forensic work, that distinction is central.
How quickly do people notice change
Some clients notice early relief, especially when the target is a single incident with clear triggers and a stable support system. Other cases take longer.
Chronic abuse, trafficking, family violence, detention trauma, and prolonged fear tied to immigration uncertainty usually require slower pacing. The same is true when the clinical picture includes dissociation, moral injury, panic, sleep disruption, or years of hypervigilance. In those cases, the goal is not speed. The goal is symptom reduction without sacrificing stability, daily functioning, or the client's ability to participate consistently in the legal process.
What if a session feels overwhelming
That risk needs to be addressed before trauma processing starts. A careful EMDR clinician prepares the client for activation, uses containment and grounding skills, and closes the session only after the client has returned to a manageable level of distress.
If you want a practical discussion of warning signs, timing problems, and who may need more preparation first, review this guide on whether EMDR can make things worse in some situations.
Can EMDR help if the problem is not classic PTSD
Yes. In practice, EMDR is often considered when the client presents with trauma-related symptoms that do not fit a simple single-event PTSD pattern. That includes prolonged anxiety, shame, guilt, moral injury, chronic fear, and somatic reactions tied to reminders of abuse or loss.
This is one reason the treatment comes up in immigration-related evaluations. A person seeking asylum or a hardship waiver may show impairment that stems from cumulative trauma, forced separation, religious persecution, domestic abuse, or threats against family members. The legal question is not whether the client uses textbook PTSD language. The question is how the psychological injury affects functioning, credibility, and future risk.
If you need an immigration-focused psychological evaluation that addresses trauma, PTSD, prolonged anxiety, moral injury, abuse dynamics, and hardship in a format built for USCIS or immigration court review, Pro Psychological Analysis provides evidence-based assessments designed to translate clinical findings into legally useful documentation.