After just six 50-minute EMDR sessions, 100% of single-trauma sufferers and 77% of people with multiple traumas no longer met diagnostic criteria for PTSD, according to a Kaiser Permanente finding summarized here. For immigration attorneys, that number should change how you think about mental health evidence.
EMDR is more than a wellness intervention. In the right case, with the right clinician, it can become part of a stronger forensic record. Trauma symptoms often interfere with narrative coherence, memory retrieval, affect regulation, and a client's ability to participate in preparation for asylum, T visa, U visa, VAWA, and hardship matters. The benefits of EMDR matter clinically, but they also matter legally when symptom change is documented carefully and interpreted within the realities of trauma.
Table of Contents
- The Power of Healing The Brain's Way
- What Is EMDR and How Does It Reprocess Trauma
- Key Clinical Benefits for Trauma Survivors
- Reviewing the Scientific Evidence for EMDR
- Determining Suitability for EMDR Therapy
- Documenting EMDR Outcomes for Forensic Evaluations
- A Guide for Attorneys Integrating EMDR into Case Strategy
The Power of Healing The Brain's Way
Major treatment guidelines have recognized EMDR as an evidence-based treatment for trauma-related conditions. For attorneys, that point is not academic. In asylum, T visa, U visa, and hardship matters, the court or adjudicator is more likely to give weight to treatment history when the method itself has established clinical standing.
That standing matters most when trauma symptoms interfere with the legal process. Clients with untreated posttraumatic symptoms often struggle to provide a clear chronology, stay regulated during declaration drafting, or discuss painful events without shutting down, dissociating, or becoming so distressed that the interview loses coherence. In practice, symptom reduction can improve more than emotional comfort. It can improve a client's ability to participate meaningfully in the case.
EMDR draws attention because it targets how traumatic memories continue to drive present-day distress. Many survivors do not need more pressure to retell what happened. They need treatment that addresses the intrusive images, physiological reactivity, shame, panic, sleep disruption, and avoidance that keep the trauma psychologically current. That distinction matters in immigration work, where clients may already be repeating their story across screenings, affidavits, attorney meetings, and testimony preparation.
I tell attorneys to watch for a practical question. Is the client unable to assist because the facts are weak, or because trauma symptoms are disrupting memory retrieval, concentration, and emotional control? The answer can affect case preparation, timing, and the interpretation of inconsistencies.
EMDR also has forensic relevance because change can be documented over time with ordinary clinical tools and careful narrative observation. A psychologist can describe baseline symptoms, treatment targets, functional impairment, and post-treatment changes in a way that is clinically grounded and legally useful. Used properly, that information can support opinions about past harm, current impairment, prognosis, and the client's capacity to participate in proceedings.
For a quick visual reference, this visual shorthand for the brain's processing of trauma captures the core idea. Trauma is often remembered not as settled history, but as a threat that still feels active in the present.
{kind=link}
What Is EMDR and How Does It Reprocess Trauma
EMDR stands for Eye Movement Desensitization and Reprocessing. It is based on the Adaptive Information Processing model, often shortened to AIP. The model holds that traumatic experiences can become stored in a maladaptive way, leaving the memory linked to intense emotion, bodily activation, and negative beliefs that continue to fire long after the event is over.
A useful analogy is a librarian working in a damaged archive. In ordinary memory processing, new experiences get filed where they belong. In trauma, some experiences are dropped into the wrong place, mislabeled, and left in a state of alarm. EMDR helps the brain revisit that material, sort it, and store it as something that happened in the past rather than something that is still happening now.
What happens during EMDR
EMDR is not a free-form technique. It follows an eight-phase protocol. The sequence matters because trauma processing without adequate preparation can destabilize a client.
- History taking and case formulation. The clinician identifies targets, symptoms, risk factors, and whether EMDR is appropriate now.
- Preparation. The client learns grounding, containment, and other regulation skills.
- Assessment. The therapist and client identify the image, negative belief, desired positive belief, emotions, and body sensations linked to a target memory.
- Desensitization. The client notices the target while following bilateral stimulation.
- Installation. The therapist strengthens the adaptive belief that replaces the old traumatic meaning.
- Body scan. Residual physical distress is checked and addressed.
- Closure. The session ends with stabilization.
- Reevaluation. The next session reviews what shifted and what remains.
Why bilateral stimulation matters
The most recognizable feature of EMDR is bilateral stimulation, often guided eye movements. The neurobiological explanation isn't hand-waving. A peer-reviewed review of EMDR mechanisms describes neuroimaging evidence of increased functional connectivity after treatment and notes bilateral stimulation is typically delivered through eye movements at 1-2 Hz for 20-30 seconds per set. That review also discusses findings by Santarnecchi and colleagues showing enhanced prefrontal control over trauma intrusions and reduced amygdala hyperactivity after EMDR.
For a non-clinical audience, the practical takeaway is simple. EMDR doesn't ask clients to “forget” trauma. It aims to reduce the memory's current power to trigger overwhelming emotional and physiological responses.
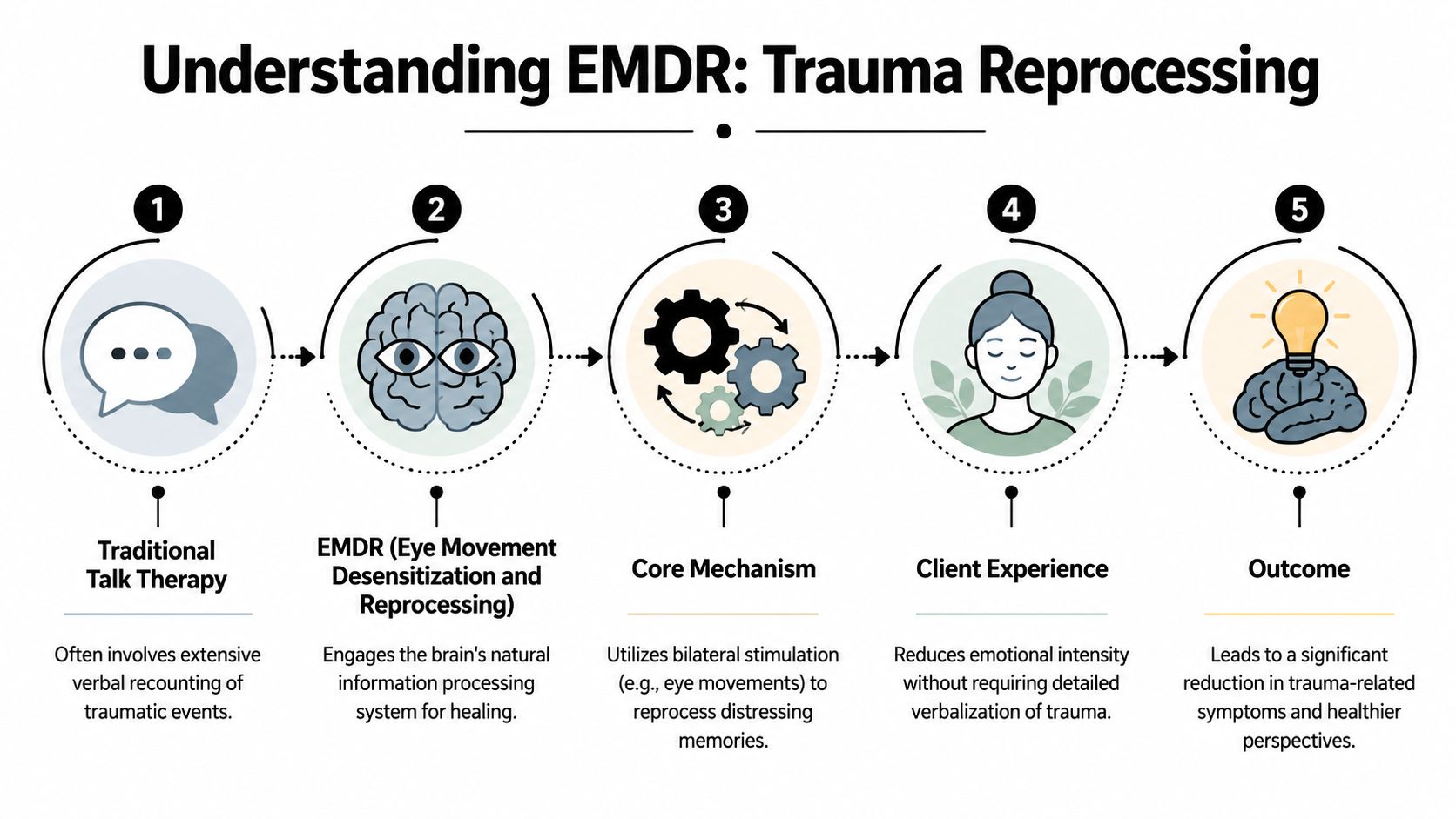
How EMDR differs from ordinary talk therapy
| Approach | Main emphasis | Typical client burden |
|---|---|---|
| Traditional talk therapy | Verbal exploration and repeated discussion | Often higher verbal detail and extended retelling |
| EMDR | Memory reprocessing through structured protocol | Less reliance on exhaustive verbal recounting |
That difference is one reason the benefits of EMDR can be especially relevant in legal populations. Some clients can discuss trauma in detail. Others shut down, become flooded, or lose coherence when pushed into repeated retelling. EMDR can offer another path.
A client's inability to narrate trauma smoothly is often evidence of trauma, not evidence against it.
Key Clinical Benefits for Trauma Survivors
Trauma symptoms often interfere with the very tasks an immigration case depends on: giving a coherent history, tolerating follow-up questions, reviewing declarations, and appearing for repeated appointments. In practice, the value of EMDR is not limited to lower symptom scores. The more relevant question for attorneys is whether treatment improves a client's ability to participate reliably in the legal process without becoming overwhelmed.
I assess these gains by function. Nightmares, panic, dissociation, shame, and intrusive memories matter clinically. For forensic purposes, what matters just as much is whether those symptoms still disrupt concentration, memory retrieval, emotional regulation, and the capacity to stay engaged during an interview. EMDR can reduce the intensity of trauma activation enough that a client is no longer controlled by reminders in the room, the wording of a question, or the expectation of having to retell painful events.
That shift is often visible.
A client seeking asylum may begin treatment in a state of constant vigilance, scanning exits, losing track of chronology, and freezing when a persecutory event is mentioned. After effective reprocessing, the same client may still feel grief, fear, or anger, but remain oriented, ask for clarification, pause appropriately, and return to the account without complete shutdown. For an attorney, that can mean more accurate fact development and fewer meetings derailed by trauma reactions.
In domestic violence, trafficking, and coercive control cases, another common change involves self-blame. Before treatment, clients often describe the abuse through rigid conclusions shaped by trauma: "I caused it," "I should have stopped it," or "It happened because I stayed." After EMDR, the memory may remain painful, but the meaning attached to it becomes more reality-based. That distinction matters in clinical records and can materially affect how an affidavit, declaration, or hardship narrative is understood.
Speed also matters in some cases, but it should be discussed carefully. As noted earlier, some EMDR studies and program summaries report substantial improvement within a limited number of sessions. That does not mean fast results should be expected in immigration matters. Many clients present with repeated trauma, ongoing threat, unstable housing, family separation, or active court stress. In those situations, progress may be meaningful but uneven. A few sessions can improve sleep, decrease reactivity, or increase interview tolerance, even when the broader trauma picture remains complex.
Here is a concise public-facing explanation worth sharing with clients who are nervous about the process:
Treatment progress is most useful legally when it increases stability without erasing the underlying trauma narrative.
The clinical gains attorneys usually find most useful are specific and observable:
- Better emotional regulation: Clients can discuss difficult facts with less flooding, less panic, and fewer abrupt breaks in attention.
- Reduced avoidance: They are more able to attend meetings, respond to preparation questions, and participate in psychological evaluations.
- Improved narrative tolerance: They can stay with the account longer, recover after activation, and provide details with fewer trauma-driven interruptions.
- Greater day-to-day functioning: Sleep, caregiving, work tasks, and basic planning often become easier to manage, which improves consistency throughout the case.
Those improvements do not prove credibility, and they do not erase inconsistencies caused by trauma, language, or time. They do something more practical. They help stabilize the client enough that attorneys and evaluators can obtain a clearer, clinically grounded picture of what happened and how the trauma continues to affect daily functioning.
Reviewing the Scientific Evidence for EMDR
Trauma treatment carries more weight in a legal record when the method has been tested against other established interventions, not just described favorably by its own proponents. EMDR meets that higher bar often enough that a forensic evaluator can discuss it in a report without sounding speculative or promotional.
Comparative evidence matters
The strongest point is comparative performance. According to the EMDR International Association efficacy summary, EMDR has performed well in randomized trials against both medication and trauma-focused CBT. For attorneys, that matters because it gives the evaluator a concrete basis for explaining why EMDR was selected for a trauma survivor whose symptoms interfere with testimony preparation, affidavit development, or participation in a psychological examination.
Therapy is not interchangeable in forensic work. A report that states "the client attended therapy" says very little. A report that identifies a trauma-focused treatment with published comparative support gives adjudicators a clearer clinical frame, especially in asylum, T visa, U visa, and hardship cases where the severity and persistence of trauma symptoms are central to the legal theory.
Endorsements support clinical credibility, not certainty
Recognition by major health bodies also matters, but it should be used carefully. Endorsement supports the view that EMDR is an accepted trauma treatment within mainstream practice. It does not prove that a particular client will improve, and it does not substitute for a competent differential diagnosis, careful symptom measurement, or a clear explanation of why the treatment fit that patient's presentation.
That distinction shows up in strong forensic writing. Clinicians should describe EMDR as an evidence-based option that was chosen for identified clinical reasons, then document what happened in treatment. Attorneys reviewing a draft evaluation should look for that sequence. Method, rationale, observed response, and remaining limitations. A practice profile for forensic psychological services can help illustrate the kind of structured clinical framing that reads well in an immigration record.
{kind=link}
What the evidence proves, and what it does not
Good science supports measured claims.
- EMDR is supported for trauma-related conditions. The research base is strongest around PTSD and closely related symptoms.
- Response varies by client. Single-incident trauma may respond faster than chronic abuse, trafficking, torture, or repeated persecution.
- Treatment success does not answer legal questions by itself. Symptom reduction is clinically useful, but it does not establish credibility, causation, or statutory eligibility.
- Timing affects forensic value. Starting reprocessing shortly before testimony or a filing deadline can help some clients and destabilize others.
In immigration cases, that last point is often where judgment matters most. I want an evaluator to be able to say not only that EMDR is scientifically grounded, but also why it was started when it was, what target symptoms were monitored, and whether treatment improved the client's ability to participate without altering the underlying trauma history.
The same summary also notes that EMDR has been recognized in treatment guidelines by respected institutions. That is useful support, but the stronger forensic move is restraint. State the level of evidence accurately, describe the client's course precisely, and separate clinical improvement from legal conclusions.
Determining Suitability for EMDR Therapy
EMDR is not the right first move for every client. The best candidates are not only “traumatized people.” They are traumatized people who have enough current stability to tolerate reprocessing without becoming more impaired.
That distinction is especially important in immigration practice. A client may have severe trauma symptoms and still not be ready for EMDR today. If the person is in acute crisis, actively using substances, psychotic, highly dissociated, or unable to use basic grounding skills, the first job is stabilization. Pushing directly into trauma processing in those cases usually backfires.
Good fit versus not yet
A practical clinical screen often sounds like this:
- Single-incident trauma with solid daily functioning: Often a strong fit for EMDR.
- Complex trauma with chronic abuse, trafficking, torture, or repeated coercion: Possibly a fit, but often only after careful preparation.
- Active instability: Usually not ready for reprocessing yet.
The distinction is not about worthiness. It is about sequencing.
Complex trauma needs a different pace
Immigration clients often present with cumulative trauma, not a single isolated event. They may carry persecution history, family separation, domestic violence, sexual assault, detention experiences, and ongoing fear of return. In these cases, EMDR can still be useful, but the clinician usually spends more time building internal resources before targeting the most painful memories.
That preparation may include affect regulation, safe-place exercises, containment work, and clear planning for what happens if the client gets flooded between sessions. A therapist who skips this stage because EMDR is “efficient” is not practicing carefully.
A simple practice overview image is a reminder of the broader point. Trauma treatment in forensic populations is not only about the protocol. It is about fit, pacing, and safety.
Questions attorneys should ask before recommending EMDR
- Is the client stable enough for reprocessing now?
- Does the clinician have experience with complex trauma, not just single-incident PTSD?
- Is there a plan for stabilization if distress increases?
- Does the provider understand that legal testimony and treatment may need coordination?
When attorneys ask those questions early, referrals improve. So do reports.
Documenting EMDR Outcomes for Forensic Evaluations
Clinical progress becomes legally useful in this context. Treatment alone does not strengthen a case. Documented treatment response can.

A strong forensic evaluation does more than state that a client attended therapy. It explains the original symptom pattern, the clinical rationale for treatment, the client's tolerance for the work, observable changes over time, and any remaining impairment. For adjudicators, that creates a more persuasive picture than generic statements such as “the client benefited from counseling.”
What useful documentation includes
The most persuasive reports usually document several layers at once:
- Baseline presentation: Intrusions, nightmares, avoidance, hyperarousal, depression, dissociation, shame, functional impairment.
- Treatment rationale: Why EMDR was selected instead of, or before, another modality.
- Course of care: Whether the client completed preparation, entered reprocessing, or required prolonged stabilization.
- Observed changes: Emotional regulation, narrative tolerance, sleep, concentration, avoidance, body-based distress, ability to engage with legal preparation.
- Remaining symptoms: Improvement does not mean full recovery.
For attorneys, this is often the sweet spot. A report can show severe trauma impact while also showing that the client is making credible, clinically consistent efforts to recover.
The gap attorneys need to understand
The literature still has a major unanswered question for immigration work. A review discussing EMDR research gaps in complex trauma contexts notes the need for more clarity on how EMDR applies to layered, cumulative trauma, especially where clients must remain stable enough for high-stakes legal disclosure. The same discussion references that 84% to 90% of people who experienced a single trauma found relief after three EMDR sessions, but that does not automatically answer what happens in polyvictimized immigration populations.
That gap should shape how a report is written. Clinicians should avoid overstating what EMDR proves in a specific asylum or trafficking case. It is more defensible to document exactly what changed and what did not.
Forensic focus: Reports should separate symptom reduction from memory fabrication concerns. The clinician's task is to describe functioning, consistency, and observed response, not to inflate certainty.
What does not work
Several practices weaken a forensic report:
| Weak approach | Stronger approach |
|---|---|
| “Client did EMDR and feels better.” | Describe baseline symptoms, treatment stage, and observed functional changes. |
| Treating symptom improvement as proof of legal credibility | Explain improvement as clinically consistent with trauma treatment, while keeping forensic conclusions disciplined. |
| Ignoring unresolved symptoms | Document residual impairment and how it still affects testimony, memory, or daily functioning. |
The benefits of EMDR become persuasive evidence only when they are documented with restraint and precision.
A Guide for Attorneys Integrating EMDR into Case Strategy
The legal question is not whether EMDR is good. The legal question is when and how to use it without undermining the integrity of the record.
A genuine challenge exists here. A discussion of EMDR and memory “updating” in relation to legal documentation highlights the concern that therapy can interact with the need for uncontaminated trauma histories. That concern is legitimate. If credibility will turn on a highly detailed chronology and the client has not yet completed a forensic evaluation, attorneys should think carefully before launching intensive trauma processing.
A practical sequencing framework
In many cases, the safest sequence is:
- Complete the forensic evaluation first. Obtain a careful trauma history and baseline symptom picture.
- Begin or continue treatment after that foundation is documented. This preserves a cleaner record of the original presentation.
- Use follow-up documentation strategically. If treatment improves functioning, submit an update or supplemental declaration where appropriate.
That won't fit every case. Some clients are too symptomatic to complete a reliable evaluation without first receiving stabilizing care. In those situations, the attorney and clinician should coordinate explicitly about goals, limits, and documentation.
What to ask the clinician
When you refer a client, ask questions that reflect both treatment and evidentiary needs.
- Has the baseline trauma narrative been documented?
- Will you distinguish preparation and stabilization from active reprocessing?
- Can you describe functional effects relevant to legal participation?
- How will you note changes without overstating certainty about memory detail?
A clinician who understands forensic work won't see those questions as interference. They will see them as necessary guardrails.
How to use the resulting evaluation
The best use of EMDR-related evidence is usually modest and targeted.
- Support impairment claims: Explain how trauma disrupted memory, affect regulation, and daily functioning.
- Support consistency: Show that the client's reactions are clinically congruent with trauma, even if disclosure has been uneven.
- Support rehabilitation, where relevant: Demonstrate that the client has engaged in evidence-based care and gained stability.
A forensic practice image captures the larger point. Immigration representation is stronger when legal and clinical work are aligned, not siloed.
{kind=link}
For attorneys handling asylum, T, U, VAWA, or hardship matters, the benefits of EMDR are most valuable when they are treated as part of a coordinated evidentiary strategy. Refer too casually, and you risk muddying the record. Refer thoughtfully, and you may help a client both heal and present a clearer, more clinically grounded case.
If you need a psychological evaluation that can address trauma with scientific rigor while staying attentive to USCIS and immigration court requirements, Pro Psychological Analysis works with attorneys nationwide on asylum, T visa, U visa, VAWA, and extreme hardship waiver cases. The practice provides evidence-based, trauma-informed evaluations designed to document symptoms, functional impairment, and clinically relevant findings in a format built for legal use.