An attorney gets the psychological evaluation back, reads it once, and feels relieved. The narrative is strong. The symptoms fit. The hardship analysis seems persuasive. Then the government asks a narrower, more dangerous question: why should anyone trust the tools behind the conclusions?
That's the moment when the validity of assessment tools stops being academic and becomes case strategy. In immigration work, a report doesn't fail only because the clinician missed something clinically important. It can also fail because the methodology looks thin, poorly matched to the client, or unsupported for the exact legal use at issue.
For attorneys, that means validity isn't just a concern for the expert. It's part of evidence review, witness preparation, and preemptive damage control. For clinicians, it means the strongest report is rarely the one with the most test names. It's the one that can explain, in plain language, why these instruments, with this client, in this setting, support the opinions offered.
Table of Contents
- The High Stakes of Evidence in Immigration Law
- The Core Pillars of Assessment Validity Explained
- Key Distinctions Face Concurrent and Predictive Validity
- Selecting Defensible Tools for Immigration Evaluations
- Reporting Validity Evidence in Medico-Legal Reports
- Common Pitfalls in Assessment and How to Avoid Them
- Frequently Asked Questions on Assessment Validity
The High Stakes of Evidence in Immigration Law
A Request for Evidence that questions the basis of a psychological evaluation can change the whole posture of a case. What looked like a supporting exhibit suddenly becomes a document that needs defending. The attorney now has to explain not only the client's condition, but also why the assessment process deserves confidence.
In immigration matters, that pressure is amplified because the consequences are personal and immediate. A weak explanation of symptoms might be repaired with supplemental detail. A weak foundation for the instruments used is harder to fix, because it calls the evaluator's method into question.
I've seen attorneys focus on whether the diagnosis sounds persuasive while giving less attention to whether the underlying measures were appropriate for language, culture, trauma history, and the legal question. That's understandable. The narrative is what everyone sees first. But adjudicators, opposing counsel, and reviewing experts often attack method because it gives them a cleaner route to dismissing the opinions.
A report becomes more defensible when the clinician can explain why each tool was chosen, what it adds, and what its limits are.
That's why the validity of assessment tools matters so much in immigration practice. It helps attorneys spot weak reports before filing. It helps clinicians avoid overclaiming. And it gives both professionals a shared vocabulary for presenting psychological evidence as careful, bounded, and trustworthy rather than impressionistic.
When validity is handled well, the evaluation reads like disciplined forensic work. When it's handled poorly, even sound clinical observations can look vulnerable.
The Core Pillars of Assessment Validity Explained
Validity is an evidence argument
The modern view of validity didn't come from one magic statistic. A foundational milestone came from the 1954 APA Technical Recommendations summarized in the validity literature), which framed validity as evidence that a test measures what it claims to measure. That idea later developed into the current multi-evidence model, where validity rests on more than one source of support.
For immigration cases, that shift matters. A clinician cannot declare an instrument “validated” and move on. The stronger question is whether the interpretation offered in the report is supported by different forms of evidence.
Building a legal record illustrates this point. One exhibit rarely carries the whole case. The pieces need to reinforce each other. The same is true here.
- Content validity asks whether the instrument covers the domain it claims to assess.
- Construct validity asks whether the tool behaves the way it should if it is measuring the intended concept.
- Criterion validity asks whether the scores relate meaningfully to an external outcome or reference point.
If you want a refresher on broader clinical foundations before assessing legal defensibility, this overview of clinical assessment basics is a useful starting point.
Core Validity Types at a Glance
| Validity Type | Key Question It Answers | Example in Immigration Evaluations |
|---|---|---|
| Content validity | Does the instrument adequately cover the issues it claims to assess? | A trauma measure includes symptoms and experiences relevant to the client's reported exposure rather than sampling only a narrow slice of distress. |
| Construct validity | Does the tool actually measure the psychological concept the evaluator says it measures? | A measure used to support an opinion about trauma-related impairment fits with interview findings, observed behavior, and related symptom patterns. |
| Criterion validity | Do the scores relate to a meaningful external benchmark? | Test results align with a current diagnosis, functional impairment, or another credible indicator relevant to the legal claim. |
Why lawyers should care about all three
Attorneys often encounter validity only after a report is challenged. That's late. A better practice is to read the methodology section with these three questions in mind.
A content problem appears when the tool doesn't speak to the legal issue. For example, a broad symptom checklist might identify distress but add little to a narrow hardship question unless the evaluator explains the link. A construct problem appears when the clinician jumps from test scores to a legal conclusion without showing that the scores accurately reflect the claimed condition. A criterion problem appears when the report relies on scores that don't clearly connect to diagnosis, functioning, or the outcome the opinion addresses.
Practical rule: Don't ask whether a test is famous. Ask whether the report shows content fit, conceptual fit, and real-world fit.
That's the core of defensibility. The legal advantage isn't in dropping psychometric vocabulary into the report. It's in using the right framework to make the expert's reasoning harder to dismantle.
Key Distinctions Face Concurrent and Predictive Validity
Face validity helps rapport but proves little
Some instruments look persuasive because the questions appear relevant on their face. That's face validity. If a trauma questionnaire asks about fear, nightmares, startle response, and avoidance, the client and attorney may feel reassured that it obviously addresses trauma.
That perception can help with rapport. Clients are more likely to engage when the assessment seems connected to their lived experience. But face validity is weak evidence. A test can look appropriate and still fail to measure the intended construct well, or fail to support the legal inference being drawn from it.
This matters in immigration work because attractive, intuitive tools can create false confidence. A report shouldn't rely on “it looks right” reasoning. It should show why the instrument was suitable for this examinee and this opinion.
Concurrent and predictive validity serve different legal tasks
Concurrent validity and predictive validity are both forms of criterion-related thinking, but they answer different questions.
Concurrent validity asks whether a score lines up with something meaningful in the present. In practice, that may mean whether results align with the evaluator's current diagnosis, current functioning, or another present indicator gathered through interview and collateral review. This is often where clinicians support statements such as, in substance, “the testing is consistent with the symptom pattern observed during the evaluation.”
Predictive validity is more forward-looking. It matters when the legal theory depends on what is likely to happen under certain conditions. In hardship cases, for example, the issue may involve likely deterioration, inability to adapt, or expected worsening under return or separation conditions. In those settings, predictive reasoning needs particular restraint. The evaluator should tie any forecast to the data collected and avoid presenting speculation as certainty.
A simple distinction helps:
- Face validity asks whether the tool seems relevant.
- Concurrent validity asks whether the score matches what is happening now.
- Predictive validity asks whether the score helps support a future-oriented conclusion.
The mistake I see most often is treating these as interchangeable. They aren't. A measure that feels relevant to the client may help establish rapport but offer little support for forecasting. A score that aligns with current diagnosis may not justify strong predictions about future functioning unless the report explains that bridge carefully.
Selecting Defensible Tools for Immigration Evaluations
The right question is fit not prestige
The most common selection mistake is choosing an instrument because it is widely known, easy to administer, or routinely used in general practice. In forensic immigration work, those reasons aren't enough. The better question is whether the interpretation of the score fits the specific use, population, and setting. That view of validity is well stated in this discussion of validity as an argument tied to context.
That principle changes how clinicians and attorneys should think about tool choice. A measure isn't automatically valid because it has a professional manual, appears in graduate training, or has been used in many clinics. The report must justify why it fits this client's language, cultural frame, trauma background, and the legal issue under review.
Structured data can help if the interview process itself is disciplined. For attorneys reviewing methodology, it's worth understanding how a structured interview can reduce drift and improve consistency in how key topics are covered.
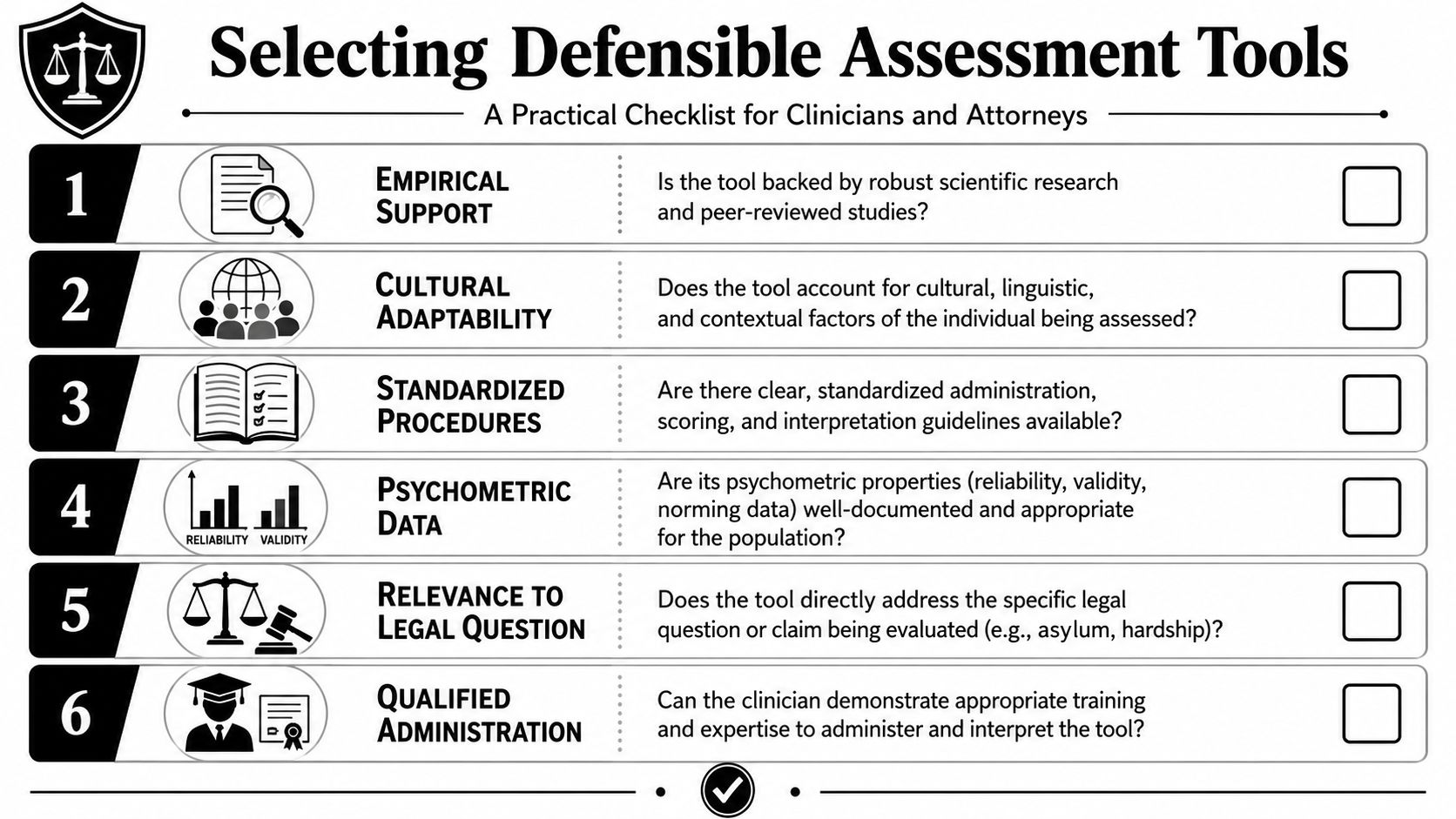
A working checklist for tool selection
Use this checklist before a clinician administers the instrument, not after the report is drafted.
- Population fit: Was the tool used with people meaningfully similar to the client in language, culture, education, and lived context?
- Purpose fit: Does the instrument help answer the actual legal question, or does it only add general clinical background?
- Administration fit: Can the evaluator explain how instructions, interpreter use, and response format affected the process?
- Scoring fit: Are the scoring rules clear enough that another qualified professional could understand how the conclusions were reached?
- Interpretive restraint: Does the tool support the opinion offered, or is the report stretching beyond what the instrument can bear?
- Corroboration: Are the test results integrated with interview data, records, observed behavior, and collateral information?
What attorneys should ask before filing
A short attorney review can expose major weaknesses early.
Ask the clinician:
Why this measure for this client?
“Because I always use it” is a poor answer. A defensible answer ties the tool to the referral question and the client's context.What does the tool add that the interview alone doesn't?
If the answer is vague, the instrument may be decorative rather than probative.What are the limitations in this case?
Strong experts identify limitations without being prompted. Weak reports often sound certain where caution is required.
If the evaluator can't explain the instrument's fit in ordinary language, that weakness will show up later in an RFE response, cross-examination, or affidavit review.
For clinicians, the lesson is simple. Selection is part of the opinion itself. For attorneys, tool choice is a screening issue, not a technical footnote.
Reporting Validity Evidence in Medico-Legal Reports
What the methodology section should do
A good methodology section doesn't merely list test names. It shows judgment. The reader should understand why the evaluator chose each instrument, what each one was intended to measure, and how the resulting data support the opinions offered.
Many reports become vulnerable when they include an inventory of measures but almost no reasoning. That invites the reader to assume the evaluator used a standard battery without tailoring it to the case.
The stronger approach is to pair each instrument with a concise rationale. The report should make clear whether the tool was used to assess symptom severity, trauma-related functioning, consistency with diagnostic impressions, or another defined purpose.
How to translate psychometrics for non-clinicians
Some psychometric terms are useful in reports, but only when they are translated. According to the Measurement Toolkit discussion of statistical assessment, commonly used indices depend on the data and the decision involved. ICC is typically used for absolute agreement, RMSE reflects average error against a reference method, and Cohen's kappa adjusts categorical agreement for chance. The same source notes that experts look for content coverage, expected relationships with related measures, and meaningful prediction of outcomes.
Most immigration adjudicators won't care about the jargon by itself. They care about what it means.
A few examples of better translation:
Instead of: “The instrument demonstrates strong agreement statistics.”
Write: “The tool has been studied for how closely its scores agree with relevant comparison methods, which supports using it as one part of the overall assessment.”Instead of: “Kappa was adequate.”
Write: “When researchers compare categorical ratings, they often correct for agreement that could happen by chance. That matters because raw agreement alone can overstate confidence.”Instead of: “Internal consistency was acceptable.”
Write: “The items function together in a coherent way, which is a basic prerequisite before relying on the score interpretation.”
If internal consistency is mentioned numerically, be careful. A commonly used screening benchmark is Cronbach's alpha above 0.70 for acceptable internal consistency, as noted in the earlier validity discussion linked above. But even that number doesn't prove the report's conclusions. It only supports one part of the measurement argument.
Sample phrasing that strengthens defensibility
The best language is direct, modest, and tied to the case.
This instrument was selected because it addresses the symptom domain relevant to the referral question and provides a structured method for comparing the client's reported experiences with recognized clinical patterns.
The test results were not interpreted in isolation. They were considered alongside the clinical interview, behavioral observations, and available records.
The assessment supports the opinion offered only within the limits of the client's language background, trauma history, and the conditions under which the evaluation occurred.
A useful template for the instruments section looks like this:
- Instrument and purpose: Name the measure and state why it was used.
- Fit to the examinee: Note any language, cultural, educational, or contextual considerations.
- Methodological support: Summarize the kind of validity evidence that makes the tool suitable.
- Limitations: State what the tool cannot establish on its own.
- Integration: Explain how the findings were weighed with non-test data.
That style tells the court or agency that the evaluator understands both psychometrics and forensic boundaries.
Common Pitfalls in Assessment and How to Avoid Them
Where reports usually become vulnerable
The most damaging errors are often ordinary ones. A clinician uses an instrument with little demonstrated fit for the client's background. An attorney assumes that a consistent test must also be accurate. A report leans heavily on one score and gives only passing attention to interview data, records, or cultural context.
One subtle trap involves benchmarks. In workforce selection settings, the U.S. Office of Personnel Management states that a validity coefficient of .30 or higher is generally considered useful for most circumstances. That doesn't mean .30 is a universal seal of approval for every psychological instrument or every forensic use. Context still governs.
For culturally responsive practice, attorneys should also understand how cross-cultural assessment affects interpretation. A score may look neat on paper and still mislead if the evaluator hasn't accounted for language, migration stress, or culturally shaped symptom expression.
How to reduce attack points before submission
A few habits prevent many of these problems.
- Separate reliability from validity: A measure can be consistent without being accurate for the purpose at hand.
- Demand contextual fit: Ask whether the instrument's use makes sense for this examinee, not just for a generic patient.
- Avoid score worship: Test data should support the clinical formulation, not replace it.
- Read certainty carefully: Conclusions should match the strength of the data. Inflated language creates openings for challenge.
- Document the process: Administration conditions, translation issues, record review, and observational findings matter.
This video gives a practical overview worth reviewing with those concerns in mind.
Reports are hardest to attack when the evaluator shows restraint, acknowledges limits, and explains why the chosen methods fit the legal question.
Frequently Asked Questions on Assessment Validity
Can a clinically useful test still be a poor legal choice
Yes. A tool can help treatment planning and still be poorly matched to a forensic immigration question. Legal defensibility depends on fit between the instrument, the client, and the opinion being offered. If the report can't explain that fit, the test may add more vulnerability than value.
Is one strong instrument enough
Usually not. In high-stakes work, a single score rarely carries enough weight by itself. The more defensible approach is convergence. Interview findings, behavioral observations, records, and carefully chosen measures should point in the same direction. When they don't, the evaluator should address the discrepancy directly rather than gloss over it.
What should an attorney do when a report already has weaknesses
Start with triage. Identify whether the weakness is in tool selection, explanation, cultural fit, administration conditions, or overstatement. Then ask whether the problem can be repaired with a supplemental declaration, additional records review, clarification of limitations, or a more tightly reasoned addendum. If the flaw goes to the core method, replacing the evaluation may be safer than defending a weak foundation.
A strong immigration case doesn't require perfect psychometrics. It requires a report that is thoughtful, transparent, and proportionate in its claims. That's what makes the validity of assessment tools a practical legal issue rather than a textbook one.
If you need immigration-focused psychological evaluations that are clinically rigorous and legally defensible, Pro Psychological Analysis works with attorneys nationwide on asylum, T visa, U visa, VAWA, and extreme hardship cases. Their team prepares evidence-based reports that translate complex clinical findings into clear support for immigration filings while maintaining confidentiality, professionalism, and close alignment with case strategy.