An attorney calls because the declaration is strong, the facts are credible, and the client clearly suffers when recounting what happened. But the file still has a gap. The case needs more than a painful story. It needs evidence that can survive scrutiny from USCIS, opposing counsel, or an immigration judge.
That's where many legal teams start asking what is clinical assessment in practical terms, not as an abstract mental health concept, but as a case-building tool. In immigration work, a clinical assessment can convert a client's subjective account into organized, evidence-based findings that speak the language of admissibility, diagnosis, causation, and functional impact.
In a forensic immigration context, the assessment is not a therapeutic intake dressed up as a report. It is a structured process for collecting, evaluating, and interpreting information from multiple sources so the final opinion is clinically sound and legally useful. Done well, it helps answer the questions adjudicators care about: What happened, what symptoms followed, how severe are they, and how confidently can those symptoms be linked to the qualifying harm?
Table of Contents
- When a Client's Story Is Not Enough
- The Anatomy of a Forensic Clinical Assessment
- Translating Trauma into a Legal Argument
- Meeting Standards for Admissibility and Impact
- How Attorneys and Clients Can Prepare for the Evaluation
- Clinical Assessments in Action Case Examples
- Frequently Asked Questions for Immigration Attorneys
When a Client's Story Is Not Enough
A client may describe detention, torture, trafficking, domestic violence, or years of coercive control with complete sincerity. The problem is that sincerity alone doesn't establish the clinical consequences of that harm. In immigration cases, the legal record often needs something more disciplined than narrative consistency.
I see this most often when an attorney has a client whose presentation is obviously trauma-related, but the file contains only a declaration, a few text messages, and maybe scattered medical notes. The attorney knows the client is struggling. The court may even sense it. Still, without a forensic clinical evaluation, the record may not clearly show diagnosis, severity, or the connection between the traumatic events and the current symptoms.
A compelling declaration tells the human story. A clinical assessment helps prove its psychological impact.
That distinction matters in asylum, T visa, U visa, VAWA, and extreme hardship cases. The legal question usually isn't whether distress exists in a general sense. The question is whether the distress can be documented in a way that is methodical, credible, and tied to the relevant legal standard.
A strong assessment also protects against a common problem. Attorneys sometimes rely on broad statements such as “the client has trauma” or “the client is depressed.” Those phrases may be true, but they are too loose to carry much evidentiary weight. A forensic evaluator has to show how the symptoms were identified, how alternative explanations were considered, and why the conclusions fit the available evidence.
Why narrative alone can fall short
Three issues come up repeatedly:
- Memory under trauma: Clients may recall events in fragments, out of sequence, or with emotional flooding. That doesn't make the account false, but it does mean the record needs careful clinical interpretation.
- Invisible symptoms: Panic, dissociation, nightmares, shame, hypervigilance, and avoidance often don't appear in ordinary documentary evidence.
- Legal burden: Adjudicators want more than empathy. They want a grounded explanation of what the symptoms mean.
When attorneys understand what is clinical assessment in this setting, they stop treating it as an optional add-on. It becomes part of case strategy.
The Anatomy of a Forensic Clinical Assessment
A forensic clinical assessment has three core pillars. It combines interview data, standardized testing, and collateral review into one coherent opinion. In immigration work, that multi-source approach matters because clinical assessment frameworks describe the process as “collecting, retrieving, evaluating, and interpreting data from multiple sources” in order to support sound conclusions and focused assessments when the history indicates a specific issue, as outlined in this clinical assessment framework.
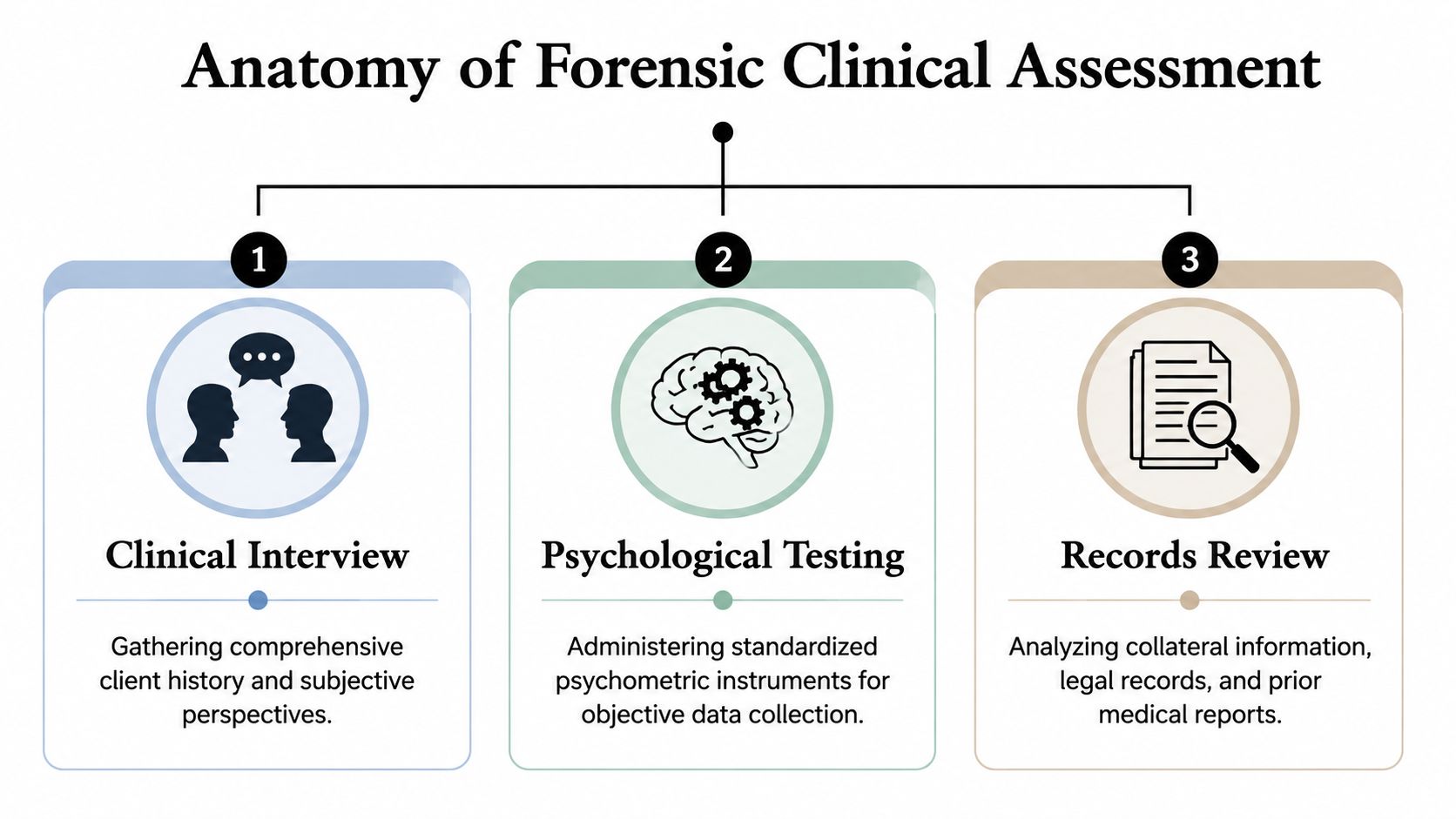
A good report doesn't stack those pieces together. It uses each one to test, refine, or confirm the others.
The interview does more than collect history
The interview is where the evaluator develops the narrative timeline and observes how the client reports symptoms. That includes trauma history, onset of symptoms, prior functioning, current impairment, and relevant family, medical, and social context.
In a forensic setting, the interview also helps answer harder questions:
- What happened before the qualifying harm
- What changed afterward
- Which symptoms fit the alleged trauma
- Whether there are competing explanations that need to be ruled in or out
Behavioral observation matters here too. The evaluator notes affect, orientation, concentration, avoidance, distress tolerance, and the way the client responds when discussing traumatic events. Those observations never replace evidence. They help interpret it.
Testing and records keep the opinion grounded
Standardized psychometric instruments add objective structure. They don't “prove” trauma by themselves, but they can measure symptom patterns and severity in a way that supports or challenges the interview findings. In immigration evaluations, that often includes trauma-related, anxiety-related, depressive, and functional impairment measures when clinically appropriate.
Then comes collateral review. That may include declarations, police reports, hospital records, therapy notes, school records, affidavits, prior evaluations, and attorney summaries. A well-done collateral review looks for consistency, timing, missing context, and contradictions that need explanation.
Practical rule: If a diagnosis appears in the report but the reader can't tell what data supports it, the assessment is incomplete.
The strongest evaluations usually have these characteristics:
| Component | What it contributes | What goes wrong without it |
|---|---|---|
| Clinical interview | Trauma history, symptom narrative, observed presentation | The report becomes generic or detached from the client's actual story |
| Psychological testing | Measurable symptom data and standardized comparison | The conclusions look purely subjective |
| Records review | External context, timeline support, corroboration | The evaluator may miss key facts or legal relevance |
What doesn't work is overreliance on any single pillar. Interview alone can become anecdotal. Testing alone can become mechanical. Records alone can become sterile. The assessment becomes persuasive when those methods converge.
Translating Trauma into a Legal Argument
A psychological report helps only if it answers legal questions in usable terms. That requires more than listing symptoms or assigning a diagnosis. The evaluator has to translate clinical findings into findings that support the case theory.

One of the most important functions of a forensic assessment in immigration law is establishing causal link and temporal sequence. General clinical literature often underemphasizes this point, but in legal settings the report needs to show that the applicant's presentation is directly attributable to the qualifying persecution, trafficking, or crime, as discussed in this analysis of clinical assessment and causality.
Diagnosis is only the starting point
A diagnosis can formalize suffering in a way that courts and agencies recognize. But diagnosis by itself is not enough. A report must also explain the meaning of the diagnosis in the context of the case.
For example, if a client meets criteria for posttraumatic stress symptoms, the legal value lies in more than naming the condition. The report should address:
- Severity: How intrusive, persistent, or impairing are the symptoms?
- Function: How do those symptoms affect sleep, concentration, work, parenting, memory, or daily safety?
- Consistency: Do the symptoms fit what clinicians would expect after the type of trauma alleged?
That consistency issue is often misunderstood. The evaluator is not vouching for every factual allegation as a witness to the events. The evaluator is assessing whether the client's reported experiences and observed symptom pattern make clinical sense together.
The report must show sequence and nexus
In many cases, the decisive issue is nexus. The attorney needs evidence showing that the mental health condition is not floating free from the underlying events. The report should map the sequence clearly.
A useful formulation often looks like this:
- Baseline before harm: What was known about the client's functioning before the persecution, abuse, trafficking, or crime.
- Exposure to qualifying events: What traumatic experiences are being evaluated.
- Onset and evolution of symptoms: When nightmares, panic, avoidance, depression, hypervigilance, or dissociation appeared and how they developed.
- Current consequences: What remains active now and how it affects functioning.
That sequencing is especially valuable when the record contains delayed disclosure, fragmented memory, or inconsistent prior descriptions. Trauma often disrupts chronology. A clinician can explain that pattern without excusing major factual problems or stretching beyond the evidence.
Courts respond to reports that do more than say a client is suffering. They respond to reports that explain why the suffering is clinically linked to the legally relevant events.
Forensic work differs from supportive therapy letters in this regard. Therapy may focus on healing. A forensic evaluation has to build a reasoned bridge from symptom evidence to legal relevance.
Meeting Standards for Admissibility and Impact
Not every mental health letter belongs in an immigration filing. Some documents are compassionate but weak. Others contain sound clinical observations but aren't structured for legal review. A forensic report has to be both clinically defensible and readable to a non-clinical decision-maker.
That is why the strongest immigration reports integrate subjective and objective material. Clinical evaluation emphasizes the patient's context and lived experience, while diagnostic investigation uses measurable methods to confirm or clarify conditions. In immigration documentation, that combined approach strengthens admissibility because it corroborates narrative claims with standardized data, as explained in this discussion of clinical evaluation and diagnostic investigation.
What makes a report persuasive
A persuasive report usually does several things well at once.
- It states the referral question clearly: The reader should know why the evaluation was requested and what legal issue it informs.
- It identifies methods: The report should specify interview procedures, testing used, and records reviewed.
- It separates data from opinion: Observations, test findings, history, and ultimate conclusions should not blur together.
- It addresses alternative explanations: If prior trauma, medical illness, substance use, or unrelated stressors may play a role, the evaluator should discuss that openly.
- It connects findings to functional impact: Judges often care less about jargon than about what the symptoms do to the client's life.
A clear structure helps. So does disciplined language. A report becomes more persuasive when it avoids advocacy rhetoric and sticks to professional reasoning.
What weakens an otherwise good evaluation
Several common mistakes can reduce impact quickly.
| Weakness | Why it hurts the case |
|---|---|
| Bare conclusions with little explanation | The adjudicator can't see how the evaluator reached the opinion |
| Advocacy language instead of clinical analysis | The report can look biased |
| No collateral review when records exist | Important inconsistencies or corroboration may be missed |
| Generic trauma language | The findings don't feel tied to the actual client |
| Confusing therapeutic and forensic roles | The purpose of the report becomes unclear |
Confidentiality also matters. Immigration evaluations involve highly sensitive facts, and attorneys should expect HIPAA-compliant handling of records, interviews, and report transmission. Ethics are not window dressing in this setting. They affect reliability.
A report is strongest when it reads like careful professional work, not like a brief written by someone with a clinical license.
That is also why attorneys should distinguish therapeutic support letters from forensic assessments. They serve different functions. One may comfort. The other must withstand scrutiny.
How Attorneys and Clients Can Prepare for the Evaluation
A common failure point looks like this: counsel sends a declaration, asks for a trauma evaluation, and expects the report to support the theory of relief. The interview goes well, but the final opinion does not answer the legal question that matters in the case. The problem usually started before the client ever met the evaluator.
Preparation shapes the usefulness of the report. In immigration practice, that means giving the clinician a clear referral question, the right records, and enough context to assess the client without drifting into advocacy or guesswork.
How to prepare the referral
The referral should tell the evaluator what the case needs proved in clinical terms. Name the form of relief, identify the alleged harm, and specify the practical questions the report should address. In an asylum case, that may mean evaluating trauma symptoms and explaining how they affect memory, disclosure, or testimony. In a hardship matter, it may mean documenting the qualifying relative's psychological condition and functional impairment under likely separation or relocation scenarios.
Records matter because they let the evaluator test consistency, clarify timing, and avoid building an opinion on one interview alone. Send the materials that fix the timeline and show prior disclosures. That often includes the client declaration, affidavits, relevant medical or counseling records, police or court records, prior immigration filings, and a short attorney memo identifying disputed issues or evidentiary gaps.
Practical details also belong in the referral. Flag language needs, literacy limits, hearing or cognitive concerns, safety issues, and any reason the client may have trouble discussing certain events. Cultural context belongs here too. Symptom expression is not uniform across communities, and standardized tools do not always capture distress accurately in refugee or survivor populations. Attorneys who want a thoughtful overview of that issue can review guidance from Respect International.
Attorneys vetting an evaluator should ask direct questions:
- Forensic experience: Has the clinician completed evaluations for asylum, T visa, U visa, VAWA, or hardship cases?
- Methods used: Does the opinion rest on clinical interview, record review, and collateral information when available, rather than a single conversation?
- Interpreter practices: Does the evaluator use qualified, neutral interpreters instead of relatives or friends?
- Role discipline: Will the clinician stay within psychological expertise and avoid offering legal conclusions?
Those questions save time later. They also reduce the risk of getting a report that sounds polished but does not hold up under scrutiny.
How to prepare the client without coaching
Client preparation should reduce confusion, not shape testimony. I tell attorneys to set expectations with plain language. The evaluator is there to assess, document, and explain. The client does not need to sound persuasive. The client needs to be accurate.
That usually means covering four points before the appointment:
- Explain the purpose: The meeting is a forensic evaluation, not ongoing treatment, even if the interviewer is respectful and trauma-informed.
- Set expectations about the process: The client may be asked for dates, sequence, prior disclosures, current symptoms, and daily functioning.
- Normalize trauma reactions: Crying, shutting down, forgetting details temporarily, or needing a break can occur during difficult interviews.
- Protect interpretation quality: Family members should not interpret. Neutral language access improves accuracy and protects the integrity of the evaluation.
A short warning helps. Some clients expect the evaluator to already know their whole story from the legal file. Others assume they should keep answers brief unless asked for more. Both assumptions can limit the usefulness of the interview. Clients should know that careful follow-up questions are normal and that detail matters.
Cultural presentation also affects preparation. Some clients describe trauma through headaches, stomach pain, exhaustion, or other bodily symptoms rather than through psychological labels. Others minimize distress out of shame, fear of authority, loyalty to family, or concern that disclosure could affect their case. If counsel flags those patterns early, the evaluator can examine them carefully and translate them into findings that are clinically sound and legally useful.
Clinical Assessments in Action Case Examples
The easiest way to understand what is clinical assessment in immigration practice is to look at how it changes the record. The examples below are anonymized composites drawn from common referral patterns, not named case studies.
How the assessment changes the record
In an asylum case, the legal file may already contain a detailed declaration about political persecution. The weak point is often credibility under pressure, especially when the client recalls events out of order. A forensic evaluation can document trauma-related memory fragmentation, hypervigilance, nightmares, and avoidance, then explain why the symptom pattern is clinically consistent with the reported persecution. The report doesn't decide the asylum claim. It helps the adjudicator understand why a traumatized person may testify the way this client does.
In a U visa matter, the issue may be substantial harm after a qualifying crime. Here the assessment can clarify the depth of psychological injury by documenting panic, depressive symptoms, fear of retaliation, functional impairment, and the way the symptoms disrupted work, parenting, or daily mobility. That changes the file from “the client was upset after the crime” to a clinically reasoned account of enduring harm.
In an extreme hardship waiver, the focus often shifts to the qualifying relative rather than the applicant. The assessment can examine how separation, relocation risk, caregiving burden, prior trauma history, or medical vulnerability interacts with current psychological functioning. What matters is not dramatic language. What matters is a disciplined explanation of why the hardship would be serious in this family's circumstances.
A quick comparison helps:
| Case Type | Primary Role of Assessment | Key Finding to Establish |
|---|---|---|
| Asylum | Corroborate trauma effects and explain symptom consistency | Psychological harm linked to persecution |
| T, U, or VAWA | Document abuse or crime-related mental health consequences | Severity and causal connection to qualifying harm |
| Extreme Hardship | Evaluate impact on qualifying relative | Functional and emotional hardship in concrete terms |
Sometimes the assessment doesn't introduce a new fact. It gives clinical structure to facts already in the record, which can be just as important.
What doesn't work in these cases is a generic letter saying the client “appears traumatized.” The assessment has to answer the legal problem the case presents.
Frequently Asked Questions for Immigration Attorneys
Common practice questions
How long does an evaluation and report take?
Timing depends on the referral question and the record. A single-issue case with limited documentation can move quickly. A case involving complex trauma, inconsistent prior statements, interpreter coordination, or extensive medical and criminal records takes longer because the clinician has to sort out what supports the legal theory and what weakens it.
Ask about timing before you file, not after. In immigration practice, the primary issue is usually not speed alone. It is whether the report can be completed with enough care to hold up if USCIS, ICE counsel, or the court examines the methods and reasoning.
Is the information confidential?
Yes, but with clear forensic limits. The client should be told who retained the evaluator, why the evaluation is being done, who is expected to read the report, and how the information may be used in litigation or adjudication.
That conversation matters. Clients often assume a forensic evaluation works like treatment. It does not. The purpose is to form and communicate an opinion for a legal case.
Can the evaluation be done virtually?
Often yes. Remote evaluations can work well when the client has a private setting, stable technology, and reliable interpreter access if needed.
Virtual work is not automatically the best choice. In some matters, in-person evaluation gives better observational data, reduces confusion during interpretation, and helps the clinician assess concentration, affect, and distress with fewer barriers. The right format is the one that produces the most reliable information for the legal question at issue.
What is the difference between a consulting expert and a testifying expert?
A consulting expert helps counsel evaluate case theory, identify missing records, and decide whether a referral is likely to add probative value. A testifying expert writes with the expectation that every method, inference, and limitation may be challenged under cross-examination or reviewed by the court.
That distinction affects drafting. A report prepared for filing should be written for hostile reading as much as supportive reading.
Why does statistical rigor matter in a psychological report?
Because legal decision-makers are asked to rely on the clinician's methods, not just the clinician's credentials. In practice, that means the evaluator should use accepted assessment methods, describe the limits of any testing, avoid overstating certainty, and explain how the conclusions were reached.
Attorneys do not need a statistics lecture. They do need to know whether the evaluator is grounding opinions in established clinical science rather than intuition alone. The broader methodological framework is discussed in research on clinical statistics from the National Center for Biotechnology Information, but the practical question in an immigration case is simpler: can the evaluator explain the reasoning in a way that is clinically sound and legally useful?
What should I look for in a final report?
Look for a report that answers the referral question in plain terms a judge or officer can follow. It should state what records were reviewed, what methods were used, what the client reported, what the clinician observed, how diagnoses were considered, and why competing explanations were accepted or rejected. It should also connect the clinical findings to the legal issue, whether that is past persecution, trauma-related impairment, abuse-related harm, or hardship to a qualifying relative.
If your firm needs immigration-focused psychological evaluations, Pro Psychological Analysis provides evidence-based assessments for asylum, T visa, U visa, VAWA, and extreme hardship cases, with reports designed to translate clinical findings into legally useful documentation for USCIS and immigration court.