You're preparing a filing. Your client has finally disclosed thoughts of not wanting to live, or has described fear, hopelessness, and collapse after abuse, trafficking, persecution, or the threat of removal. The legal theory may be strong, but the record is thin. A brief therapy note saying the client is “depressed” won't carry much weight if USCIS or the court needs to understand severity, current risk, and the connection between trauma and functional impairment.
That's where a suicidal ideation assessment becomes more than a clinical exercise. In immigration work, it can become evidence. Done correctly, it translates subjective suffering into structured findings, explains risk in language adjudicators can follow, and supports the legal question at issue, whether that is asylum, VAWA, a T visa, a U visa, or an extreme hardship waiver.
Table of Contents
- Why Suicidal Ideation Assessment Is Critical in Immigration Cases
- Beyond a Single Question The Components of a Defensible Assessment
- Validated Instruments The Tools of the Trade
- From Assessment to Action Risk Formulation and Safety Planning
- Documenting for Impact What USCIS and Courts Look For
- Adapting Assessments for Trauma Culture and Telehealth
- A Strategic Tool for Your Strongest Case
Why Suicidal Ideation Assessment Is Critical in Immigration Cases
The attorney has a declaration, treatment records, and a brief therapist letter stating the client is depressed and overwhelmed. Then USCIS issues an RFE, or the case heads to merits, and the record still does not answer the questions that decide credibility and weight. How serious is the risk. What facts support that opinion. How does the mental health evidence connect to hardship, trauma, abuse, or fear of return.
That gap is common in immigration cases. Clinical concern alone is not enough. The assessment has to produce evidence that is specific, organized, and tied to the legal issue in dispute.
A proper suicidal ideation assessment does more than confirm distress. It distinguishes passive death wishes from active suicidal thinking. It clarifies plan, intent, prior attempts, preparatory behavior, protective factors, and recent escalation. Just as important, it shows the evaluator used a method that another professional, an adjudicator, or a court can follow and scrutinize.
This is significant in immigration practice, as many clients present with trauma histories, coercive relationships, detention exposure, family separation, chronic uncertainty, or fear of removal. Those conditions can intensify hopelessness and perceived entrapment. In a legal record, that context matters only if the evaluator documents how it affects current risk and functioning.
Why a standard psych note often fails
A short treatment note may describe anxiety, insomnia, crying spells, or panic. That may be clinically useful for ongoing care, but it often carries limited evidentiary weight. USCIS officers, immigration judges, and trial attorneys usually need a clearer record of three things:
- What was assessed: suicidal ideation, plan, intent, prior behavior, triggers, protective factors, and resulting impairment
- How it was assessed: a documented interview process, with clear observations and clinically grounded reasoning
- Why it matters legally: a direct connection between the findings and the hardship claim, trauma claim, abuse history, or consequences of return or separation
A defensible report shows the basis for the opinion, not just the conclusion.
In practice, that distinction often decides how persuasive the report will be. A vague letter invites doubt. A structured assessment gives the factfinder a timeline, identified risk factors, observed symptoms, and a reasoned professional judgment.
Where this becomes decisive
In asylum matters, suicidal ideation can help document the psychiatric impact of persecution, torture, sexual violence, or the anticipated effects of return. In VAWA, T visa, and U visa cases, it can support the record on abuse, coercion, victimization, and ongoing psychological injury. In hardship waivers, it may help establish that separation, relocation, or prolonged instability would likely produce serious mental health deterioration in the qualifying relative or applicant, depending on the claim.
The trade-off is straightforward. Broad statements are faster to draft, but they rarely hold up under close review. Specific assessments take more work, yet they are far more useful when the government asks how the clinician reached the opinion and whether the risk is current, foreseeable, and clinically significant.
What persuades is specificity. If the record says only that the client is struggling, the adjudicator is left to fill in the missing facts. A well-documented suicidal ideation assessment reduces that problem and makes the mental health evidence much harder to dismiss.
Beyond a Single Question The Components of a Defensible Assessment
The weakest approach is the one many non-clinicians assume is enough: “Are you thinking of hurting yourself?” If the client says no, the inquiry ends. That isn't a defensible assessment. It's a screening fragment.
A legally useful suicidal ideation assessment works more like a careful investigation. Screening is the first signal. Structured interviewing gathers the facts. Risk formulation integrates those facts into a professional opinion that can support action and documentation.
Screening identifies the initial concern
Screening is the tip-off, not the full case file. The evaluator determines whether suicidal thoughts may be present and whether immediate escalation is necessary. This stage should be brief but direct.
A robust screen doesn't reduce the issue to a yes or no answer. Validated approaches measure dimensions such as frequency, controllability, closeness to an attempt, distress, and impact on functioning. The C-SSRS also grades severity by the highest ideation category present, which makes findings more granular than an unstructured interview, as described in the SIDAS overview from the Australian National University.
Structured interviewing develops the evidence
After screening, the evaluator has to ask follow-up questions that courts would expect a serious clinician to ask. That includes timing, triggers, duration, what the client means by “I don't want to wake up,” whether thoughts are intrusive or deliberate, and whether they have moved toward any plan or preparation.
This stage is where many reports become persuasive or collapse. A client may say, “I think about disappearing.” That could reflect despair, passive death wishes, or active suicidal intent. Without clarification, the statement is too ambiguous to carry evidentiary weight.
A solid structured interview usually addresses:
- Nature of the thoughts: Passive death wish, active ideation, method-specific thinking.
- Control and intensity: Whether the thoughts feel fleeting, recurrent, or hard to resist.
- Movement toward action: Planning, access to means, rehearsal, or preparatory behavior.
- Context: Trauma reminders, detention fears, family separation, court dates, or abusive contact.
Practical rule: If a report doesn't distinguish ideation from plan, intent, and behavior, an attorney should assume opposing review will find that gap.
Risk formulation is the final opinion
Risk formulation is where the clinician answers the question the legal record needs answered. Not “Is the client distressed?” but “What is the level and nature of current suicide risk, what factors drive it, and what reduces it?”
That opinion should synthesize multiple sources, rather than repeating the client's words. In immigration cases, this matters because the evaluator may need to explain why the client's presentation is consistent with trauma even when disclosure is fragmented, hesitant, or inconsistent on minor details.
Here's the practical difference:
| Weak approach | Defensible approach |
|---|---|
| Asked one direct question | Used screening plus structured follow-up |
| Recorded a symptom | Measured severity and context |
| Gave a diagnosis only | Linked findings to risk and functioning |
| Stopped at narrative description | Produced a reasoned clinical opinion |
A one-question approach might satisfy a rushed intake. It won't hold up as strong forensic documentation.
Validated Instruments The Tools of the Trade
A report lands on your desk two days before filing. The client says, “I think about not wanting to be here,” and the evaluation notes only “suicidal ideation present.” For treatment, that may trigger follow-up. For USCIS, asylum adjudication, or a VAWA filing, it leaves avoidable holes. The legal question is not whether distress exists. It is whether the evaluator used a recognized method, applied it correctly, and documented findings in a way that supports a reasoned opinion.
Attorneys do not need psychometric training. They do need to recognize when an instrument adds evidentiary value and when a test name is included only to make a report look technical.

What each instrument contributes
The Columbia-Suicide Severity Rating Scale (C-SSRS) is useful because it separates ideation, plan, intent, and suicidal behavior in a structured sequence. That distinction carries weight in immigration cases. An officer or reviewing court may read “suicidal thoughts” very differently from “recurrent ideation with preparatory behavior” unless the report makes the difference explicit.
The Beck Scale for Suicide Ideation (BSS) can help when the evaluator needs a formal inventory to supplement the interview. I find it most useful when the client has difficulty describing internal states, gives sparse answers, or minimizes symptoms in narrative form but responds more consistently to structured items.
The Suicidal Ideation Attributes Scale (SIDAS) is often the better fit when the report needs a clear description of severity. It examines frequency, controllability, perceived closeness to an attempt, distress, and interference with daily functioning. Those domains translate well into legal writing because they connect symptoms to day-to-day impairment rather than leaving the record at “thoughts present.”
For attorneys who want a closer look at how standardized measures support defensible opinions, this overview of the validity of assessment tools is a useful companion.
Why validation matters in an immigration report
Validated instruments do not replace clinical judgment. They give the evaluator a recognized framework for exercising it. That difference affects how persuasive the report will be when reviewed outside a clinical setting.
USCIS and immigration courts are not grading the evaluator on bedside manner. They are assessing whether the opinion is anchored in a method that other qualified professionals would recognize as legitimate. A validated tool helps show that the clinician did more than record a symptom and attach a diagnosis.
The SIDAS is a good example. Its published validation data allow an evaluator to discuss severity with more precision than a purely impressionistic narrative allows. That is important because the evaluator may need to explain why the client's symptoms indicate clinically significant risk or functional impairment even if the client disclosed them hesitantly, inconsistently, or through an interpreter. A score never decides the case by itself, but it can support a clearer and more defensible explanation.
What attorneys should look for in the tool section of a report
A strong report does more than list acronyms. It shows why the measure was chosen, whether it fits the referral question, and how the result informed the ultimate opinion.
Look for:
- A named instrument: C-SSRS, SIDAS, BSS, or another recognized measure is identified clearly.
- A stated purpose: The evaluator explains why that tool was used for this client and this referral.
- Actual interpretation: The score or findings are explained in plain language.
- Integration with the record: Test findings are considered alongside interview content, observed behavior, trauma history, and case-specific stressors.
- Attention to limits: The report addresses factors such as translation, literacy, dissociation, guardedness, or cultural idioms that may affect responses.
A test score is not the opinion. In a legally defensible immigration evaluation, it is one piece of the foundation for the opinion.
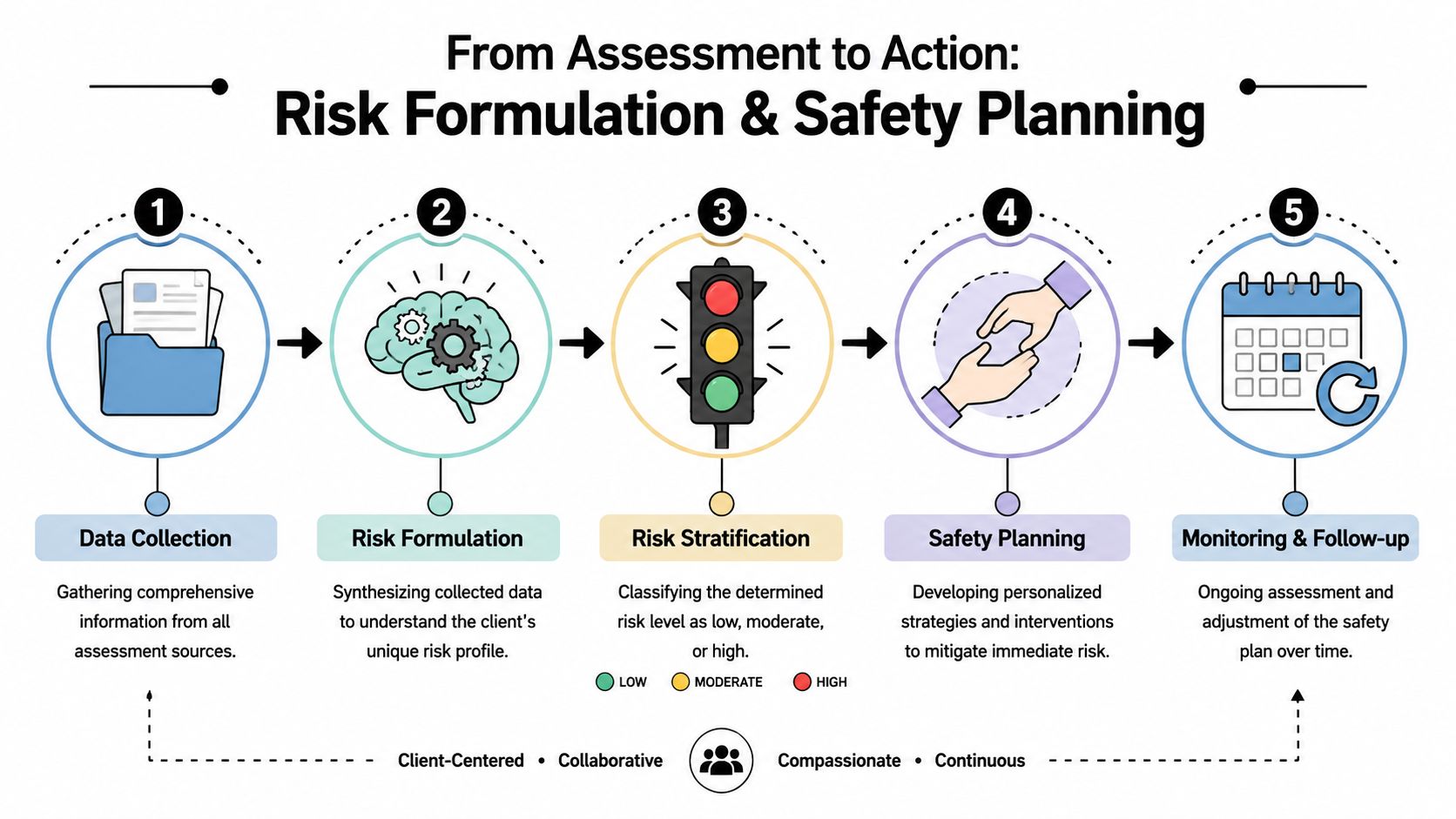
From Assessment to Action Risk Formulation and Safety Planning
An assessment that ends with “client endorses suicidal ideation” is unfinished. The clinician has to decide what the findings require. In practice, that means moving from description to risk formulation, then from formulation to safety planning.
Early in this phase, I want the legal team to understand one point clearly. A person can have suicidal ideation without needing emergency hospitalization, and a person can deny ideation while still presenting acute risk. The evaluator's job is to weigh the whole picture.
What belongs in a risk formulation
A sound formulation combines static factors, dynamic factors, and protective factors. It doesn't merely count symptoms.
Static factors may include prior attempts or a longstanding trauma history. Dynamic factors include current stressors such as contact with an abuser, a recent denial, detention fear, housing instability, or escalating isolation. Protective factors might include children, religious beliefs, treatment engagement, future goals, or supportive relatives.
Guidance on suicide risk assessment is explicit that the process should evaluate ideation, plan, intent, behavior, available means, preparatory acts, timing, location, and prior attempts. It also treats preparatory behavior and access to lethal means as high-signal indicators that can shift the response from outpatient management to hospitalization, according to the Minnesota suicide risk assessment guidance.
How findings change the intervention
The intervention has to match the risk picture. That's where many reports for legal cases become too passive. They describe serious symptoms but say nothing about what the clinician did.
A practical ladder looks like this:
- Lower acute risk: Collaborative safety planning, crisis contacts, coping steps, and removal or restriction of means where possible.
- Increased concern: More frequent follow-up, family or support involvement with consent, tighter monitoring, and active coordination of care.
- High acute risk: Emergency evaluation, hospitalization, or continuous observation when indicated.
For clinicians working within legal cases, the threshold question is often whether there is current intent, preparation, or inability to maintain safety outside a higher level of care. Attorneys should also understand related obligations around mandatory reporting requirements, because risk management decisions can affect confidentiality expectations and case logistics.
A useful visual summary appears below.
What good safety planning looks like
Safety planning is not “call 911 if worse.” It should be individualized, realistic, and documented. The plan should reflect what the client can realistically do, whom they trust, what warning signs they recognize, and what barriers exist.
| If the report says this | It should also show this |
|---|---|
| Client has recurrent suicidal thoughts | Frequency, triggers, and coping steps |
| Client has access to means | Whether means restriction was discussed |
| Client is isolated | Whether supportive contacts were identified |
| Risk is elevated | Concrete monitoring or referral steps |
That kind of documentation matters clinically. It also matters legally because it shows the evaluator understood the seriousness of the presentation and responded appropriately.
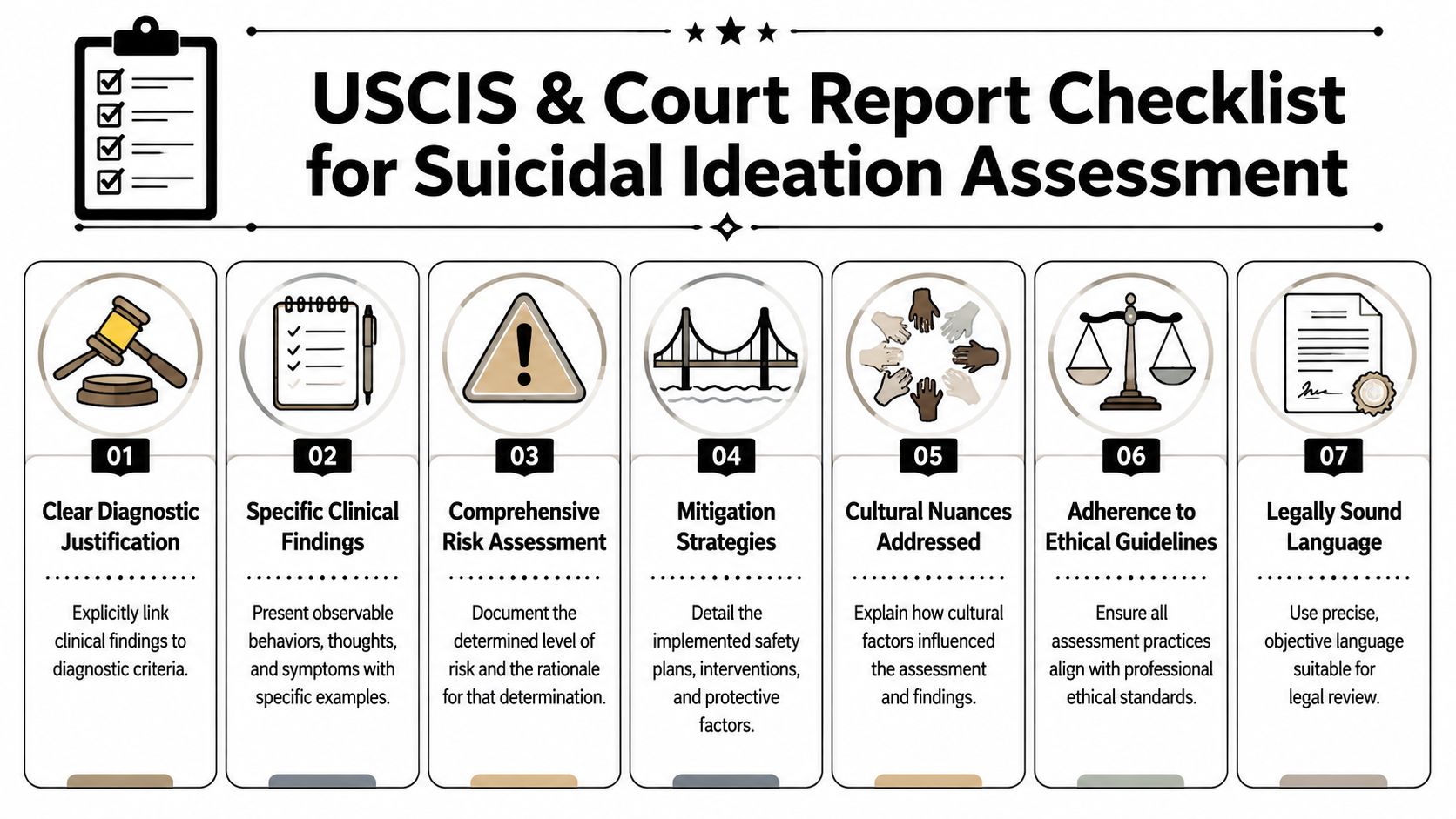
Documenting for Impact What USCIS and Courts Look For
The report has to do more than sound compassionate. It has to read as reliable evidence. USCIS officers, immigration judges, and government counsel look for specificity, internal consistency, and a clear connection between findings and the legal issue.
That means the report should begin with the referral question, identify the data sources, describe the methods used, and explain how the evaluator reached the conclusions. It should also make the trauma-to-symptom nexus unmistakable. If the client's suicidal thinking intensified after threats, rape, family separation, detention experiences, or fear of return, that sequence needs to be stated plainly.
Weak wording and stronger wording
The fastest way to improve an immigration mental health report is to replace vague language with observable, supportable findings.
“The client is very depressed and has had suicidal thoughts” won't carry the same weight as “The client endorsed recurrent suicidal ideation during structured assessment, reported limited control over these thoughts during periods of trauma activation, and described functional impairment consistent with severe psychological distress.”
Here are practical comparisons:
| Weak language | Stronger language |
|---|---|
| Client feels hopeless | Client described persistent hopelessness linked to fear of removal and separation from children, with associated sleep disruption, withdrawal, and recurrent thoughts of death |
| Client denies being suicidal today | Client denied current intent during the interview, but the evaluator noted recent statements reflecting desire not to live, marked constriction in affect, and contextual stressors requiring continued monitoring |
| Trauma affects mental health | Symptoms emerged in temporal relation to reported abuse and intensified when the client discussed return to the country of feared harm |
The report elements that make findings usable
A court-ready report usually includes these pieces:
- Referral clarity: Why the evaluation was requested and what legal question it addresses.
- Data sources: Interview dates, record review, collateral information if available, and instruments used.
- Behavioral observations: Affect, thought content, psychomotor signs, concentration, and credibility-relevant observations stated carefully.
- Risk analysis: Ideation, plan, intent, behavior, means, protective factors, and current level of concern.
- Nexus statement: How the symptoms relate to the client's trauma, abuse, persecution, or family circumstances.
- Functional impact: Effects on sleep, work, parenting, concentration, social engagement, and treatment needs.
What adjudicators tend to distrust
They tend to discount conclusory statements. They also notice when reports overreach. If the evaluator states that the client is at “extreme risk” but documents no plan, no intent, no behavior, and no rationale, the opinion becomes easier to attack.
What works better is disciplined language. State what is supported. Explain what remains uncertain. Document the reasons for the opinion.
Clinical writing tip: Precision is more persuasive than intensity. A measured opinion with a clear rationale usually survives scrutiny better than dramatic wording.
In immigration settings, the strongest reports don't just say the client suffers. They show exactly how that suffering presents, how it was assessed, and why it matters to the adjudicator's decision.
Adapting Assessments for Trauma Culture and Telehealth
Many immigration clients won't disclose suicidal ideation in a clean, linear way. Some are ashamed. Some fear hospitalization. Some worry that any admission of suicidality will harm the case, affect custody, or trigger police involvement. Others come from cultural contexts where psychological pain is described through bodily symptoms, spiritual language, or indirect expressions of burden.
That's why a good suicidal ideation assessment has to be trauma-informed and culturally responsive from the start. The evaluator should slow the pace, explain confidentiality and its limits, and avoid jumping into blunt questions before enough trust exists to get meaningful answers.
When denial doesn't end the inquiry
A denial is data. It isn't always the end of the analysis. Clinical guidance emphasizes that evaluators should remain alert even when a client denies ideation, using observable cues, context, intent, plan, access to means, and behavioral indicators to understand risk. The same guidance also recognizes that standard tools can miss culturally mediated expressions of distress according to the VA suicide risk assessment reference guide.
In practice, that means listening for statements such as “my family would be better without me,” “I want God to take me,” or “I can't continue if they deport me.” Those statements may not sound like direct admissions, but they often require careful follow-up.
Cultural and trauma adaptations that help
Some adjustments improve both accuracy and defensibility:
- Use culturally accessible language: Ask about wanting to disappear, not waking up, or feeling life is no longer bearable if direct suicide terminology creates shame or confusion.
- Attend to context: A flat denial given in the presence of a family member, interpreter concern, or visible fear shouldn't be treated the same as an open and relaxed denial in a private setting.
- Respect pacing: Trauma survivors may disclose risk in layers. Pressing too hard too fast can shut down the interview.
Clinicians should also handle consent carefully, especially when the work is being done for a legal case. Before a remote or in-person evaluation, it helps to establish expectations using clear informed consent procedures that address confidentiality, emergency response, and the role of the evaluation in litigation.
Telehealth requires added structure
Remote assessments can be clinically sound, but only if the evaluator plans for emergencies. At minimum, the clinician should verify the client's physical location, obtain an emergency contact when appropriate, confirm privacy, and discuss what happens if acute risk emerges during the session.
A simple telehealth checklist includes:
- Location verification: Know where the client is at the time of the session.
- Privacy check: Confirm who is present and whether the client can speak freely.
- Emergency pathway: Identify local emergency options if the risk escalates.
- Support access: Determine whether a trusted person can be reached if needed.
The practical point is straightforward. If the method of assessment ignores trauma, culture, or telehealth realities, the findings may be incomplete. In immigration work, incomplete findings can weaken both safety planning and the evidentiary value of the report.
A Strategic Tool for Your Strongest Case
A strong suicidal ideation assessment does something a generic mental health letter can't. It turns distress into evidence that is structured, supportable, and relevant to the legal standard. That matters when the case depends on showing extreme hardship, the impact of persecution, the consequences of abuse, or the danger of family separation.
For attorneys, the strategic value is clear. A defensible evaluation identifies the presence and severity of suicidal thinking, separates ideation from plan and intent, documents functional impairment, and explains the nexus between the client's immigration circumstances and psychological risk. It also shows that the clinician followed a serious method rather than offering a broad opinion unsupported by assessment.
The best immigration reports are never assembled as an afterthought. They are built with the same care as the legal brief itself. When the mental health evidence is rigorous, the case theory becomes easier to prove and harder to dismiss.
If your firm needs immigration-focused psychological evaluations that translate trauma findings into clear, admissible evidence, Pro Psychological Analysis provides structured, evidence-based reports for asylum, VAWA, T visa, U visa, and extreme hardship matters, with clinically rigorous documentation designed for USCIS and immigration court review.