An immigration attorney sends over a VAWA evaluation referral late in the day. During the interview, the client describes coercive control, isolation, and threats tied to her status. Then another fact surfaces. Her U.S. citizen child has been left alone overnight more than once while the abusive partner disappears for days. The child also has untreated medical needs.
At that moment, the legal strategy and the safety duty stop feeling separate. The clinician is thinking about mandated reporting requirements. The attorney is thinking about case exposure, client trust, and whether a report will trigger panic about family separation. The client is often thinking one thing above all: if I tell the truth, will I lose my child or get deported?
That is the core dilemma in immigration work. Abuse disclosures are often central to the case, but the same facts can activate reporting duties under state law. If the team handles that badly, the client may shut down, the record may become inconsistent, and genuine danger can remain unaddressed. If the team handles it well, the client can be protected without sacrificing clinical integrity or legal judgment. The pressure of this kind of work also takes a toll on professionals, especially those regularly hearing trauma narratives and crisis disclosures. That strain is worth monitoring in the same way we monitor client safety, particularly if your team has noticed signs discussed in this piece on vicarious trauma symptoms in helping professionals.
Table of Contents
- The Professional's Dilemma An Introduction
- Who Is a Mandated Reporter
- What Triggers a Mandatory Report
- Navigating State Law Variations
- Reporting Duties Versus Client Confidentiality
- Special Considerations in Immigration Cases
- A Practical Workflow for Reporting and Documentation
The Professional's Dilemma An Introduction
In forensic immigration practice, the hardest moments usually don't come from unclear trauma histories. They come from clear disclosures with painful consequences. A psychologist evaluating a client for asylum, a U visa, or VAWA may hear facts that support the legal claim and also trigger mandatory reporting requirements under state law.
That overlap creates a professional dilemma for both the clinician and the attorney. The attorney wants to preserve trust, avoid avoidable damage to the case, and prepare for any agency contact that may follow. The clinician has a separate legal obligation that usually can't be delegated, delayed for strategic reasons, or negotiated away by agreement.
The pressure point in immigration cases
The immigration context makes everything sharper. Many clients have already been threatened with police, courts, child welfare agencies, or deportation. Some were told by abusers that any disclosure would lead to the loss of their children. Others come from countries where state systems are corrupt, violent, or impossible to trust.
A routine warning about limits of confidentiality may not feel routine to them. It may sound like a direct threat unless the professional explains it calmly, concretely, and with cultural humility.
Mandatory reporting isn't just a legal checkbox in these cases. It's often the moment when the client decides whether the system is dangerous or survivable.
What works in real practice
What helps is early clarity. Before the substantive interview gets deep, the clinician should explain the boundaries of confidentiality in plain language. The attorney should prepare the client for that conversation rather than treating it as a side issue.
A useful framing sounds like this:
- Your information is private in most situations. That remains the default.
- Some safety issues are different. State law may require a report if certain facts are disclosed.
- A report is not a judgment that abuse is proven. It is a request for the proper agency to assess safety.
- The team will respond thoughtfully. That includes documenting carefully and explaining next steps.
When professionals avoid this conversation because they fear frightening the client, they usually make things worse. Surprise destroys trust faster than disclosure of the rule itself.
Who Is a Mandated Reporter
A mandated reporter is a person whom state law requires to report certain suspected harm to the appropriate agency. In most states, that duty attaches because of the person's profession and the information learned in that professional role. The common examples are familiar: psychologists, physicians, nurses, therapists, teachers, school staff, social workers, child care workers, and often law enforcement and clergy, depending on the jurisdiction.

Why the law puts the duty on individuals
The key point for attorneys working with clinicians is that the duty is usually personal. A supervisor can advise. Office counsel can help interpret a statute. An attorney can discuss downstream risks. But the individual reporter generally can't shift the obligation to someone else and assume the job is done.
That matters in multidisciplinary immigration work because teams often function collaboratively. A lawyer may say, "Let's think this through first." A clinic administrator may say, "Run it by compliance." Those are sensible process steps, but they don't erase the reporting duty if the legal trigger has already been met.
A practical way to think about mandated reporters is this: the state treats them as designated first observers in high-risk settings. Teachers see children repeatedly. Therapists hear disclosures. Physicians notice injuries and neglect patterns. Social workers may see living conditions directly. The law uses those vantage points to move possible victims toward investigation and protection.
Why professional observations carry weight
That role isn't symbolic. In a national child welfare dataset covering 204,414 children reported for physical abuse in 2013, reports made by professionals were 1.32 times more likely to be confirmed than reports made by nonprofessionals, and professional reporters initiated more than three-fifths of all maltreatment reports by 2014, according to U.S. child welfare research published by the National Library of Medicine.
For immigration attorneys, that has two implications.
| Practical issue | What it means |
|---|---|
| Clinical observations matter | A psychologist's description of what was seen, heard, and documented may carry substantial weight once a report is made. |
| Training matters | Professionals need to separate observation from interpretation, because the report may influence a larger protective process. |
Practical rule: If your role makes you a mandated reporter, the obligation belongs to you personally even when you're part of a larger legal team.
That doesn't mean clinicians should act impulsively. It means they should know whether they fall within the statute where they practice, and attorneys should assume that many of the experts they retain do.
What Triggers a Mandatory Report
The trigger for a mandatory report is usually not certainty, proof, or a completed investigation. It is reasonable cause or reasonable suspicion. That standard is lower than many professionals instinctively want, especially when they are trained to be careful, neutral, and evidence-based.

Reasonable suspicion is the threshold
Guidance on child-abuse reporting consistently emphasizes that the legal trigger is reasonable cause or reasonable suspicion, not proof, and that reporters should act on observable indicators and disclosures without waiting for certainty because the law is designed to move potential victims into protective investigation quickly, as described in this overview of school mandatory reporting standards.
The most useful analogy for attorneys and clinicians is a smoke alarm. A smoke alarm doesn't prove the house is on fire. It signals enough concern to require action. Mandatory reporting works the same way. The reporter is not the final fact finder. The reporter identifies a credible safety concern and sends it to the agency assigned to investigate.
That distinction matters because many professionals hesitate for the wrong reason. They think, "I don't know enough yet," when the law asks a different question: "Do you have enough to reasonably suspect?"
Common trigger areas in practice
In real casework, the main trigger areas usually look like this:
- Child abuse or neglect: A child discloses being hit, left unsupervised, sexually touched, denied food, or deprived of needed medical care.
- Abuse of an older adult or dependent adult: The concerns may involve physical abuse, neglect, exploitation, or unsafe caregiving conditions, depending on state law.
- Serious risk of harm: This can include imminent danger to self or others where another legal duty may also apply.
A few examples show where professionals often get stuck:
- A disclosure without visible injury. A child says a caregiver hits them with a belt. The lack of bruising doesn't eliminate the reporting issue.
- Behavior plus context. A child presents as fearful, hypervigilant, and consistently hungry, and the caregiver's account doesn't fit the child's functioning.
- A parent disclosure during an immigration evaluation. The adult client minimizes conduct that still sounds like neglect or unsafe supervision.
You don't need to prove abuse occurred. You need to recognize when the facts are enough to require a report.
What doesn't work is conducting an internal mini-trial. Clinicians sometimes over-interview in an effort to become certain. Attorneys sometimes want to delay action until they can assess case risk. Both responses can create legal exposure and can distort the factual record. The safer approach is disciplined judgment, prompt consultation if needed, and timely reporting to the correct agency.
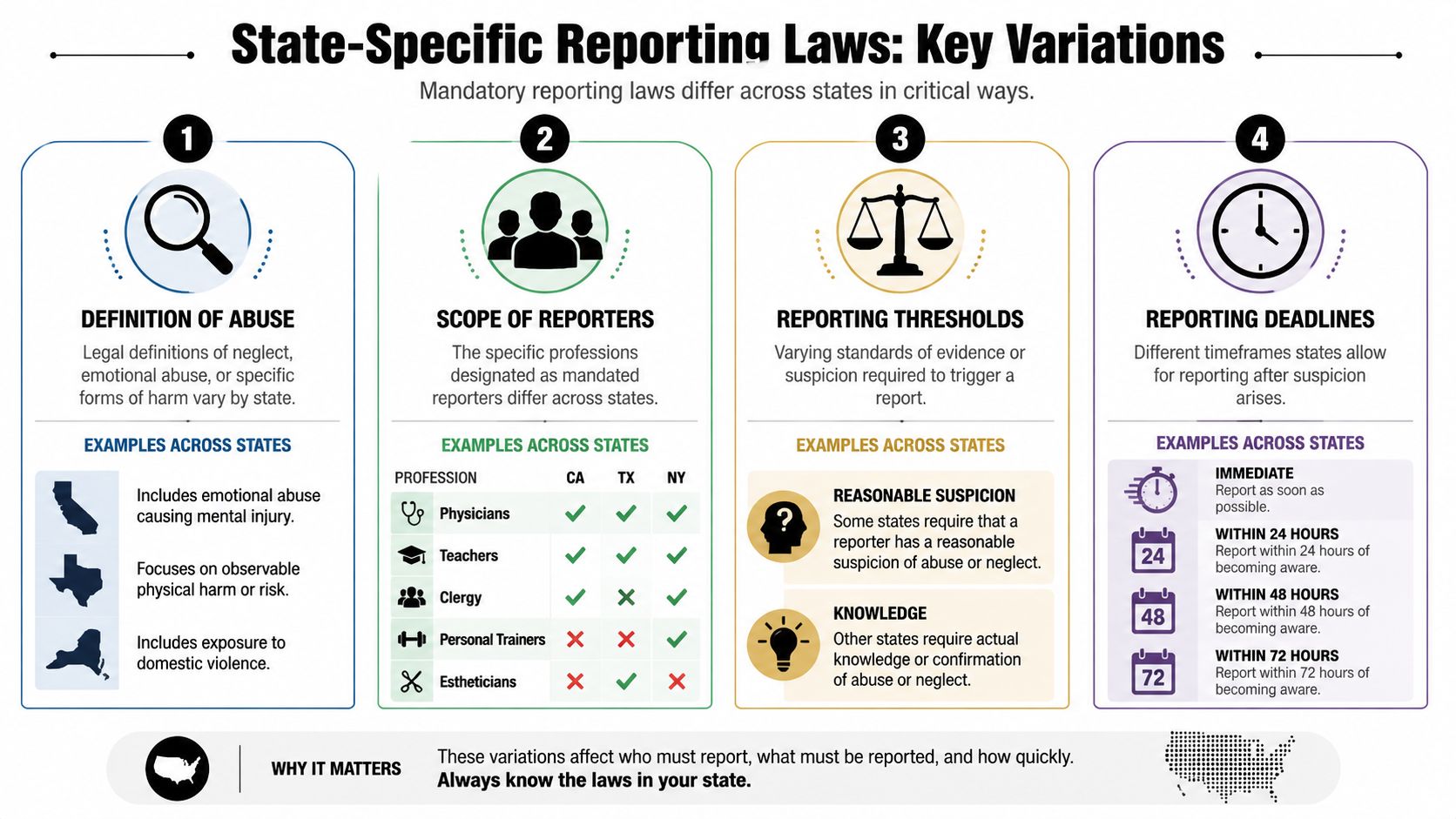
Navigating State Law Variations
Many attorneys assume there is one national set of mandatory reporting requirements. There isn't. These duties are creatures of state law, and the differences are large enough to change what must be reported, who must report, when the report must be made, and how much discretion the professional has.
There is no single national rulebook
A 2024 policy review found that only 17 U.S. states had universal mandatory reporting policies, while training was required for some or all mandated reporters in only 20 states, which underscores how fragmented the policy environment remains, as summarized in this 2024 review of mandated reporting policy variation.
That variation shows up in several ways:
| Variable | What changes by state |
|---|---|
| Who must report | Some states limit the duty to named professions. Others impose broader duties. |
| What counts as reportable | Definitions of abuse, neglect, exploitation, and exposure vary. |
| Reporting deadlines | Some jurisdictions require immediate reporting. Others allow a short written follow-up period or use different timing language. |
| Training and process | Some states require formal training. Others place the duty on professionals without much procedural support. |
For immigration practitioners, state variation has one very practical consequence. You can't rely on what was true in your last case, your law school memory, or another state's compliance training.
How to verify the law quickly
When a case may trigger reporting, use a short verification routine:
- Check the current statute. Read the actual state law for the client's location and the professional's location if they differ.
- Confirm the reporter category. Don't assume every psychologist, evaluator, contractor, intern, or advocate is treated the same way.
- Locate the reporting agency instructions. State child welfare or adult protective services websites often specify hotline, written form, and timing rules.
- Review licensing guidance. Professional boards sometimes publish clearer practice guidance than the statute alone.
- Document the legal basis for the decision. A brief note about the applicable standard helps later if the report is questioned.
The weakest compliance habit is informal reliance on office folklore. The best one is current, state-specific verification done every time the issue arises.
Reporting Duties Versus Client Confidentiality
Many clinicians and attorneys talk about reporting and confidentiality as if they are in conflict. In practice, they're usually not. Mandatory reporting laws are built as exceptions to ordinary confidentiality rules. That includes many situations where a clinician would otherwise protect information under professional ethics or health privacy law.
Confidentiality has built in exceptions
For clinicians, the right question isn't "Will reporting violate confidentiality?" The right question is "Does this situation fall within a legally recognized exception that requires or permits disclosure?" When the answer is yes, the disclosure is part of lawful practice, not a departure from it.
That is why informed consent matters so much at the beginning of an evaluation. Clients need a concrete explanation that confidentiality is broad but not unlimited. This is especially important in forensic and immigration-related assessments, where the client may already feel exposed by the process itself. A careful intake process, like the one described in these informed consent procedures for psychological services, reduces shock when a hard issue arises later.
A useful script is simple: "Most of what you share stays private. If you tell me facts that trigger a legal duty to report abuse or immediate danger, I may have to make that report." Clients usually handle that better than professionals expect, provided the explanation is calm and honest.
Child and adult reporting frameworks are not interchangeable
Many teams make avoidable mistakes by treating "mandatory reporting" as one unified rule. It isn't. Child reporting and adult or older-adult reporting often operate under different statutes, different triggers, and different confidentiality assumptions.
A recent APS brief notes that all states except New York have mandated reporters for adult protective services, and 15 states use universal reporting for adults, a framework that is separate from the child-abuse system, according to the NCEA and NAPSA mandated reporting brief.
That distinction matters in mixed-population practice. A clinician may evaluate a trafficking survivor who is also a parent, caregiver, or dependent adult victim. One encounter can raise more than one reporting framework, each with different rules. Attorneys shouldn't assume that advice developed around child abuse reporting transfers cleanly to elder abuse, dependent adult abuse, or APS reporting.
The safest approach is population-specific analysis, not a one-size-fits-all confidentiality script.
Special Considerations in Immigration Cases
The standard advice on mandatory reporting requirements often sounds straightforward. See something concerning, report it. In immigration cases, that advice is incomplete because it ignores the client's lived reality.
Why immigrant clients may fear disclosure
Many immigrant clients don't hear "protective investigation" when a professional mentions a report. They hear "government," "records," "separation," and "loss of control." Some have mixed-status families. Some have prior contact with family regulation systems. Some were explicitly threatened by abusers who said police, CPS, or courts would take the children if the client ever spoke up.
In VAWA, U visa, T visa, and asylum-related work, those fears often sit inside the abuse pattern itself. Abusers weaponize legal vulnerability. They threaten false reports. They tell the survivor nobody will believe them because of language barriers, undocumented status, poverty, or prior trauma. By the time the client reaches counsel or a psychologist, silence has often become a survival strategy.
That is why a blunt "I may have to report that" can do damage, even when legally accurate. It may shut down the interview and leave the professional with a thinner, less reliable history.
How attorneys and clinicians can work together
The better approach is coordinated and specific.
- Prepare before the interview. Attorneys should flag foreseeable reporting issues for the evaluator when referral materials already suggest child endangerment, dependent-adult abuse, or acute safety concerns.
- Explain the system in plain terms. Clients need to know what a report is, what it is not, and who may receive it.
- Separate immigration strategy from safety duty. The clinician should not shape reporting decisions around case advantage. The attorney should not ask the clinician to hold a report that state law requires.
- Plan for the aftermath. If a report may occur, the legal team should think ahead about declarations, corroborating records, custody concerns, and how to address the issue consistently if USCIS or the immigration court later sees related documents.
A common mistake is assuming that reporting automatically undermines the client's case. Sometimes the opposite is true. A well-documented response to an unsafe situation can strengthen credibility because it shows the record was handled responsibly and contemporaneously. Other times, the report may create complications that require careful legal management. Either way, denial and delay rarely help.
Immigration cases also raise logistical issues that ordinary outpatient practice doesn't. The client may move between states. The children may be in another household. The abuse may have occurred in more than one jurisdiction. The evaluator may be licensed in one state and interviewing a client in another. Those facts don't erase reporting duties. They make jurisdictional analysis more important.
The most effective teams tell the client the truth early, preserve dignity during the process, and avoid false reassurance. Clients can tolerate difficult facts better than confusion.
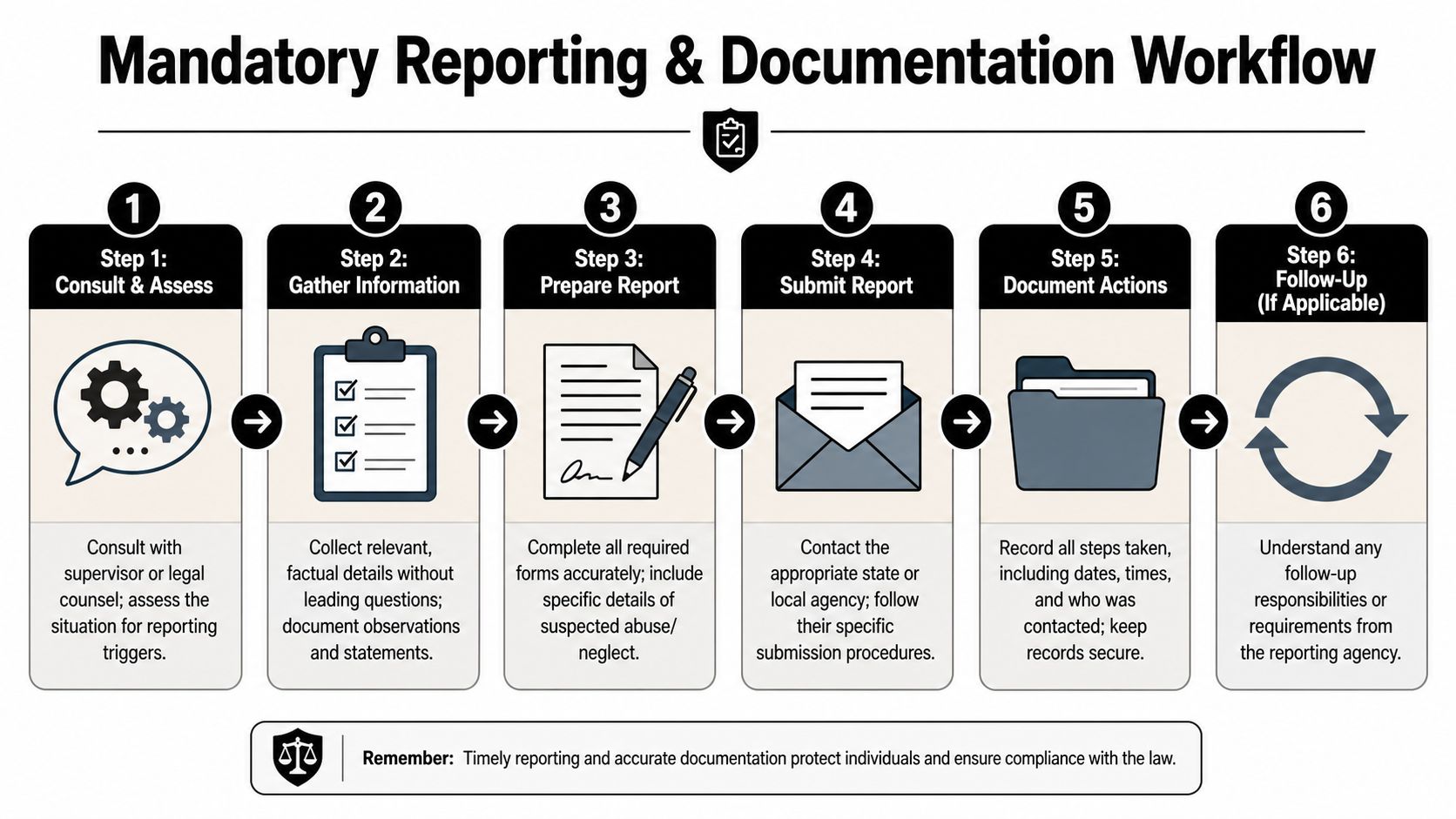
A Practical Workflow for Reporting and Documentation
When a concern surfaces, professionals need a workflow they can execute under pressure. The goal is not perfect certainty. The goal is a defensible, lawful, and humane response.
A field tested sequence
Use this order when the facts may trigger a report:
- Pause and identify the legal issue. Ask whether the disclosure concerns child abuse or neglect, adult or dependent-adult abuse, or immediate risk.
- Consult quickly if needed. A supervisor, agency protocol, or legal counsel can help with interpretation, but consultation should support timely action rather than become a delay tactic.
- Make the report to the correct agency. Follow the state-specific hotline and written follow-up process if required.
- Tell the client what happened. Use direct language. Don't sound defensive or vague.
- Coordinate with counsel appropriately. In immigration matters, the attorney needs to understand the existence of the report and any likely records trail.
This training video is a useful supplement for staff who need a visual walk-through of response steps.
Documentation that helps rather than harms
The quality of the note often determines whether the process remains clear or turns messy. Good documentation is factual, chronological, and restrained.
- Record observations, not conclusions. Write what the client said, what you observed, and what action you took.
- Use quotation marks only for exact statements. If the child or adult used a specific phrase, capture it precisely.
- Avoid advocacy language in the clinical note. The note isn't the place to argue the immigration case.
- Log reporting details. Include date, time, agency contacted, report method, and any reference number if one is provided.
- Preserve related records carefully. A disciplined file structure matters, especially where reports may intersect with forensic materials and declarations. This overview of medical documentation practices in legal cases is a useful reference point for teams building cleaner records.
Good reporting notes are specific enough to be useful and narrow enough to avoid speculation.
What doesn't work is overexplaining motive, diagnosing credibility in the reporting note, or mixing clinical impressions with legal argument. The note should let an outside reader see the factual basis for the decision without guessing how the professional got there.
The professionals who handle these moments best usually do three things consistently. They explain limits of confidentiality before deep disclosure begins. They verify the applicable law instead of relying on memory. They document with precision after acting.
When an immigration case involves trauma, abuse, or vulnerability, the clinical record has to do two jobs at once. It must protect the client's dignity and withstand legal scrutiny. Pro Psychological Analysis provides immigration-focused psychological evaluations for asylum, T visa, U visa, VAWA, and hardship cases with the clinical rigor, documentation discipline, and attorney collaboration these high-stakes matters require.