You receive the evaluation a week before filing. The report looks polished. It cites standardized instruments, lists diagnoses, and uses the right clinical vocabulary. But the conclusions don't fit your client's account. The client describes terror, shame, family pressure, and culturally shaped ways of expressing distress. The report reads as if the only possibilities are exaggeration, personality pathology, or weak credibility.
That mismatch is not a minor drafting issue. In immigration practice, a flawed psychological report can damage the case it was supposed to strengthen. It can dilute trauma evidence, distort the meaning of symptoms, and hand opposing counsel or an adjudicator an apparently objective document that points in the wrong direction.
For attorneys handling asylum, T visa, U visa, VAWA, and hardship matters, understanding cultural bias in psychological testing is no longer optional. You don't need to become a psychometrician. You do need to know when an evaluation is clinically sound, when it is merely formal-looking, and how to challenge it before it harms the record.
Table of Contents
- When a Psychological Report Creates More Problems Than It Solves
- Defining Cultural Bias in Psychological Testing
- The Sources of Bias From Test Creation to Clinical Judgment
- How Biased Testing Can Jeopardize Immigration Cases
- Mitigation Strategies for Ethical and Defensible Evaluations
- How Attorneys Can Identify and Challenge Biased Test Evidence
- Partnering for Fair and Accurate Assessments
When a Psychological Report Creates More Problems Than It Solves
An attorney sends a client for evaluation because the case needs trauma documentation. The client has survived detention, threats, sexual violence, trafficking, or prolonged coercive control. The report returns with neat labels and high scores, but it treats unfamiliar affect, guardedness, indirect communication, or somatic distress as evidence of inconsistency rather than context.
I've seen this problem in several forms. A trauma survivor from a collectivist background is described as “dependent” because family obligation is mistaken for pathology. A client who expresses depression through headaches, body pain, and exhaustion is treated as vague or non-psychiatric because the evaluator expects a Western style of emotional disclosure. A guarded asylum applicant is framed as evasive without meaningful discussion of fear, shame, interpreter dynamics, or prior persecution by authorities.
Why the report becomes dangerous evidence
A weak report can be ignored. A biased report is worse. It can actively reshape how a decision-maker views the client.
Consider what happens when the evaluator:
- Overstates pathology: culturally normative behavior gets recast as disorder.
- Misses trauma expression: the report minimizes symptoms because the client doesn't describe distress in the expected style.
- Forgets the legal question: the evaluator writes for a clinic chart, not for asylum, hardship, or victim-based immigration relief.
- Assumes test objectivity: scores are treated as self-explanatory, even when the measures are a poor fit for the person being tested.
Practical rule: If the report feels out of sync with the client's lived reality, don't assume the client presented poorly. First ask whether the evaluator used the wrong framework.
The legal problem is straightforward. Immigration adjudicators often give psychological evidence weight precisely because it appears specialized and neutral. When that evidence is culturally distorted, the neutrality is an illusion. The report may still look professional while undermining nexus, hardship, credibility, trauma impact, or the seriousness of psychiatric impairment.
Defining Cultural Bias in Psychological Testing
Cultural bias in psychological testing is a systematic error. The scores vary because of the test-taker's culture rather than actual ability or the trait the evaluator intends to measure, which undermines validity, as described in this discussion of cultural bias and construct validity.
A simple analogy helps. If you use a ruler designed for flat wood to measure a coiled spring, you may get a number, but the number doesn't answer the right question. The problem isn't that measurement occurred. The problem is that the tool and the target don't match.

The legal problem behind the clinical language
For attorneys, the key issue is reliability. If a test is culturally biased, the resulting score may say more about language, familiarity, acculturation, social assumptions, or normative mismatch than about trauma, cognition, personality, or symptom severity.
That is why a culturally informed evaluator does not stop at reporting scores. The evaluator explains whether the instrument is appropriate for this client, in this language, for this legal purpose. That same concern sits at the center of good cross-cultural assessment practice.
The three technical failure points
The literature identifies three core forms of bias.
Construct non-equivalence
This is the deepest problem. The trait itself may not mean the same thing across cultures. Concepts like independence, suspiciousness, dissociation, anxiety, or even intelligence can be organized differently depending on cultural context. If the construct doesn't travel well, the score can't be interpreted in the same way.
Item or content bias
Sometimes the problem sits inside the question. The wording may assume cultural knowledge, use poor translation, rely on idioms, or introduce nuisance factors unrelated to the trait being measured. A client may miss the item not because of pathology or low ability, but because the item is foreign, vague, or culturally loaded.
Sampling bias
A test's norms depend on who was included in the standardization sample. If the “normal” comparison group does not adequately represent people like your client, the resulting interpretation becomes fragile. The evaluator may be comparing your client to a population that was never meant to serve as a fair benchmark.
A score is only as useful as the population and assumptions behind it.
For legal strategy, these distinctions matter. They help you identify whether the flaw is in the definition of the trait, the wording of the questions, or the norm group used to interpret results. Those are different objections, and they call for different cross-examination.
The Sources of Bias From Test Creation to Clinical Judgment
A clinician can administer a technically polished test and still produce a report that misleads the court. In immigration work, that usually happens because bias entered long before the evaluator formed an opinion. It entered in test development, in norming decisions, in translation choices, and then again in the examiner's clinical judgment.
The history still matters
Early U.S. psychological testing was tied to eugenics, racial hierarchy, and immigration control. According to the APA historical chronology excerpt, early testing practices ranked groups by supposed innate worth and used culturally loaded procedures to justify exclusionary policies, including segregation, sterilization, and discriminatory immigration enforcement.
For attorneys, the point is not historical outrage. The point is legal caution. Psychological testing in the United States was not built on a neutral foundation, and some of its assumptions still show up in modern reports dressed in technical language.
Where bias enters a modern evaluation
The first problem is normative mismatch. Many commonly used instruments were developed and standardized on populations that do not reflect the linguistic, educational, migration, and trauma backgrounds seen in immigration practice. If the comparison group is poorly matched, labels such as average, high, defensive, or clinically significant become less reliable.
The second problem is administration. A test can be acceptable on paper and still become distorted in practice if instructions are simplified inconsistently, if an interpreter paraphrases symptom language, or if the evaluator ignores how education level and acculturation affect test-taking style.
Then clinical judgment adds another layer of risk.
I see this often in forensic review. An evaluator expects eye contact, rapid disclosure, linear memory, and emotionally explicit answers. An asylum seeker with torture exposure or chronic coercive control may present with guardedness, fragmented recall, or flattened affect instead. A weak evaluator reads that as evasiveness, poor credibility, or personality pathology. A stronger evaluator asks whether culture, trauma, and interview context offer the better explanation.
Attorneys reviewing methodology should also understand the basics of assessment tool validity in forensic and clinical settings. A report is only as persuasive as the instrument, the administration conditions, and the examiner's reasoning.
Clinical bias is not always over-pathologizing
Some evaluators make the opposite error. They overcorrect for culture and dismiss genuine symptoms as normal cultural difference. I treat that as the over-accommodation paradox.
In practice, this can be just as damaging as over-pathologizing. A clinician may minimize PTSD, depression, dissociation, or cognitive impairment because the client comes from a community where distress is expressed somatically, indirectly, or through spiritual language. The report then understates impairment, hardship, or trauma-related functional loss. For an immigration attorney, that is not a subtle academic problem. It can undercut nexus, credibility, past harm, future risk, and the severity of psychological injury.
Types of Bias and Their Manifestations
| Type of Bias | Description | Example in an Immigration Context |
|---|---|---|
| Construct bias | The trait being measured is not culturally equivalent | An evaluator interprets strong family obligation as dependent pathology |
| Item bias | A question depends on culturally specific language or assumptions | A client misunderstands an item because the wording carries unfamiliar social meaning |
| Sampling bias | Norms are based on an unrepresentative reference group | A trauma scale is interpreted against a norm group unlike the applicant's background |
| Language bias | Translation or interpreter use alters meaning | Symptom nuance is lost because distress terms have no close equivalent |
| Examiner bias | The clinician's assumptions shape administration or interpretation | Guardedness is framed as deception rather than trauma-related caution |
| Over-accommodation | The evaluator minimizes real pathology to avoid appearing culturally insensitive | Severe trauma symptoms are dismissed as culturally typical reactions |
One practical takeaway matters more than the label. Attorneys should ask where the error occurred. Was the problem in the test itself, the norm group, the translation, the interview method, or the clinician's interpretation? Those are different weaknesses, and they support different objections, rebuttal opinions, and cross-examination points.
Standardized testing is not neutral by default. In immigration cases, it earns credibility only when the evaluator can explain why this tool, with this client, under these conditions, supports a fair interpretation.
How Biased Testing Can Jeopardize Immigration Cases
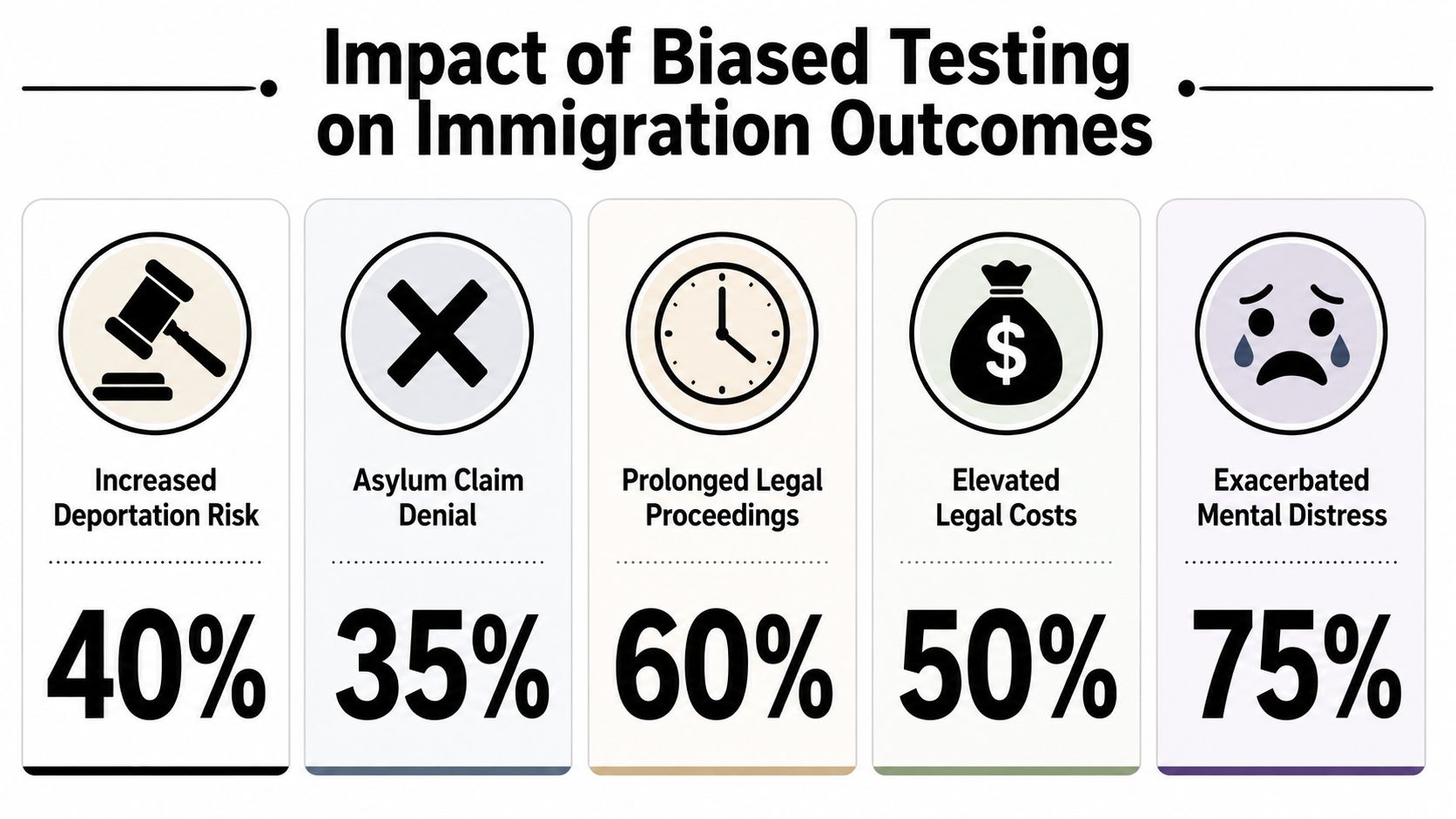
The legal damage appears when biased clinical interpretation enters the record as if it were objective fact. In immigration cases, that can affect credibility, severity, nexus, hardship, rehabilitation, and future risk.
At the center of the problem is this: cultural bias can produce systematic errors that “underestimate potential” and “over-pathologize symptoms” for minority groups, while clinicians may also generate false positives and false negatives when they misread culturally shaped behavior, according to the Joint Educational Standards discussion and related summary of diagnostic disparities.
What legal harm looks like in practice
In an asylum case, a biased report may label trauma responses as personality pathology. That doesn't just create a bad diagnosis. It can shift the narrative from persecution-related injury to preexisting character defect.
In a VAWA or trafficking case, the evaluator may minimize coercive control because the client doesn't describe abuse in familiar psychological language. The report then misses the central legal theme: domination, fear, entrapment, and impaired autonomy.
In an extreme hardship case, the evaluator may understate psychiatric impact because the client presents with stoicism, somatic complaints, or culturally shaped restraint rather than overt emotional breakdown. The hardship argument becomes thinner than the actual clinical picture.
A short visual may help frame the consequences attorneys often see in practice.
Why this becomes a credibility problem
Psychological evidence often influences how adjudicators read testimony gaps, memory fragmentation, delayed disclosure, and inconsistent affect. If the evaluator misunderstands cultural distress patterns, the report can convert understandable trauma presentation into “inconsistency,” “manipulation,” or “lack of insight.”
That is why biased testing is not an academic flaw. It is prejudicial evidence. It can make a vulnerable client appear less harmed, more disordered, less believable, or less impaired than the underlying facts support.
The wrong evaluation doesn't merely fail to help. It can teach the fact finder the wrong way to read the client.
Mitigation Strategies for Ethical and Defensible Evaluations
A defensible immigration evaluation starts before the first test is administered. The evaluator should know the legal question, the client's language and education profile, the likely trauma history, and whether standardized measures will clarify or distort the picture.
In my practice, the strongest reports use testing as one tool, not the spine of the opinion. If an instrument has limited cross-cultural applicability, I either narrow the inference or choose a different method. If a symptom scale is included, the interpretation has to account for literacy, acculturation, interpreter effects, migration stress, and culturally shaped ways of describing distress.
Interview method matters just as much as test selection. A careful structured or semi-structured interview often yields better information about chronology, coercion, avoidance, dissociation, and functional decline than a hurried battery of scores. Attorneys who want a practical frame for that difference can review this explanation of what a structured interview is.
Good evaluators also address item fairness and construct validity directly. Differential Item Functioning, often shortened to DIF, is one way psychometricians examine whether test items operate differently across groups even when the underlying trait is similar. In an immigration case, that concern is practical. If language, culture, or migration experience changes how a client understands or answers an item, the score may reflect measurement error rather than psychopathology.
There is a second risk that attorneys should watch for. Over-accommodation can be just as damaging as over-pathologizing. Some clinicians become so cautious about cultural bias that they discount genuine PTSD, depression, panic, cognitive impairment, or trauma-related inconsistency as merely “cultural.” That mistake produces a polite but clinically weak report. The result is underdiagnosis, understated impairment, and missed links between symptoms and the legal standard.
Several practices predict trouble.
- Test-first evaluations: the clinician begins with a battery before establishing language proficiency, trauma history, or the client's way of communicating distress.
- Generic cultural language: the report mentions culture in passing, but the methods, score interpretation, and diagnostic reasoning stay unchanged.
- Interpreter use without method analysis: the evaluator notes an interpreter but does not discuss translation limits, dialect differences, or how interpreted testing may affect reliability.
- Score dumping: the report recites scales and elevations without explaining what the measures can support in this case.
- Over-accommodation: the clinician dismisses clinically significant symptoms to avoid appearing culturally insensitive.
A stronger report shows its work. It explains why each method was chosen, states what the testing can and cannot establish, and ties clinical findings to the specific immigration issue at stake. It also separates culturally normative behavior from trauma symptoms without assuming every unusual presentation is either pathology or culture. That is how an evaluation becomes harder to impeach and more useful to counsel.
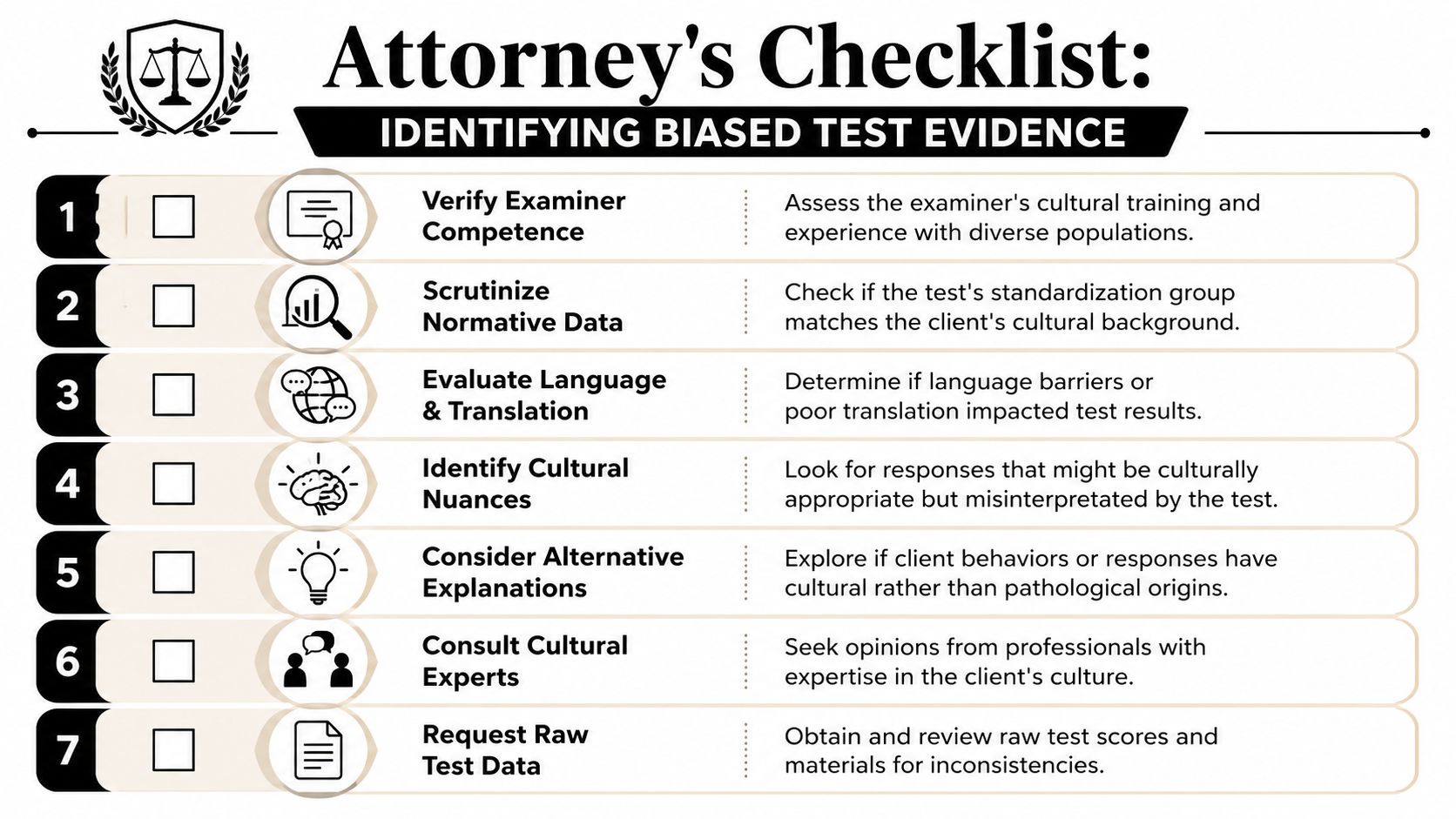
How Attorneys Can Identify and Challenge Biased Test Evidence
Most attorneys don't need to debate psychometrics at a doctoral level. They need a practical review framework. Start with the report itself. The language, omissions, and interpretive leaps usually reveal more than the test names.
Red flags in the report itself
Look for these warning signs:
- No cultural formulation: the report gives demographic facts but no analysis of language, migration history, acculturation, religion, family structure, or culturally shaped distress.
- Uncritical score interpretation: the evaluator reports test elevations as if the norms automatically apply.
- No explanation for test selection: there is no reason given for why these instruments fit this client and this legal question.
- Pathology without context: guardedness, somatic symptoms, indirect communication, or deference are described as clinical deficits with little cultural analysis.
- Thin interview data: the test battery does most of the work because the interview was too limited to capture trauma and context.
- No discussion of limitations: every assessment has constraints. A report that claims certainty without caveats is often less reliable, not more.
If you suspect problems, ask for raw data and scoring materials where appropriate and permitted. Ask how the examiner handled translation, whether the norms match the examinee in any meaningful way, and what evidence supports cross-cultural use of each instrument.
Questions worth asking the evaluator
These questions often expose whether the methodology was careful or automatic:
- What made this test appropriate for this client's language and cultural background?
- What norm group was used to interpret the results?
- How did you distinguish trauma-related guardedness from evasiveness or personality pathology?
- What alternative explanations did you consider before assigning diagnosis?
- How did interpreter involvement affect administration and interpretation?
- Which findings came from interview, which came from testing, and where did they conflict?
Ask the evaluator to separate observation from inference. Many weak reports blur that line.
The over-accommodation paradox
There is another risk attorneys often miss. Some evaluators know cultural bias is a serious concern, so they become reluctant to diagnose at all. They treat severe symptoms as mere cultural difference, spiritual belief, or unfamiliar style. That error can be just as damaging as over-pathologizing.
The National Academies summary archived in PubMed Central describes this problem as the over-accommodation paradox. In that pattern, clinicians' fear of being biased leads them to dismiss genuine psychiatric symptoms in minority clients as cultural beliefs. The result is under-diagnosis and failure to provide needed treatment.
For immigration cases, this matters a great deal. A report can sound respectful and still be clinically negligent. If the evaluator repeatedly explains away panic, psychosis, dissociation, major depression, or trauma symptoms as “cultural,” the report may minimize the true extent of impairment.
That gives attorneys a second challenge framework. Don't only ask whether the evaluator pathologized culture. Ask whether the evaluator used culture to avoid recognizing real psychopathology.
A careful legal review therefore has two tracks:
| Review track | What to watch for | Likely consequence |
|---|---|---|
| Over-pathologizing | Culturally normative behavior labeled disordered | Exaggerated pathology, credibility distortion |
| Over-accommodation | Genuine symptoms dismissed as cultural style or belief | Minimized harm, under-diagnosis, weaker legal showing |
The strongest challenge is usually methodological, not rhetorical. Point to missing cultural analysis, unsupported norm use, absent validity discussion, and failure to separate cultural context from psychiatric impairment. That is far more persuasive than saying the report “felt wrong.”
Partnering for Fair and Accurate Assessments
Psychological evidence can be powerful in immigration practice. It can clarify trauma, explain delayed disclosure, document functional impairment, and connect suffering to the legal standard. But it only helps when the evaluation is methodologically disciplined and culturally competent.
Attorneys should treat mental health evidence the same way they treat country conditions, medical records, and expert declarations. Scrutinize fit. Scrutinize assumptions. Scrutinize whether the methods answer the legal question for this client, not for some abstract average person.
The practical takeaway is simple. Biased evaluations usually reveal themselves through mismatched norms, poor cultural analysis, overreliance on scores, weak interviewing, or an evaluator who either pathologizes cultural difference or dismisses real illness out of fear of bias. Those are not minor technicalities. They go to weight, reliability, and fairness.
When attorney and evaluator work as real collaborators, the report becomes more than admissible. It becomes usable. It speaks the language of both clinical rigor and legal relevance, which is exactly what vulnerable clients need when the stakes are protection, status, family unity, and safety.
If you need immigration evaluations that are clinically rigorous, culturally informed, and built for legal use, Pro Psychological Analysis works with attorneys nationwide on Asylum, T visa, U visa, VAWA, and Extreme Hardship cases. The practice delivers evidence-based reports, clear diagnostic formulations, and timely collaboration designed to support strong filings and defensible testimony.