When attorneys ask whether EMDR can help a traumatized client, they usually mean symptom relief. In immigration work, that isn't the only question that matters. The harder question is whether a trauma treatment can temporarily destabilize a client, alter how they describe events, or create avoidable problems in a case where credibility and consistency are under constant scrutiny.
The short answer to can EMDR make things worse is yes, but not in the simplistic way many people fear. EMDR is generally considered a low-risk trauma treatment, and the most common negative effects are temporary negative thoughts or feelings between sessions, not physical danger, as described by Cleveland Clinic's overview of the 8-phase EMDR protocol. At the same time, temporary symptom spikes are real. For some clients, especially those processing severe trauma, distress can increase before it settles.
That distinction matters more in immigration cases than in routine outpatient therapy. A client may be preparing an asylum declaration, discussing trafficking, or recounting domestic violence in a VAWA matter. If treatment increases nightmares, emotional flooding, dissociation, or confusion around memory detail at the wrong time, the legal consequences can be significant even if the treatment remains clinically appropriate overall.
A balanced understanding of EMDR requires looking at both its benefits and its risks. For a broader clinical overview of positive treatment outcomes, see these benefits of EMDR.
Table of Contents
- Introduction
- The Before Better Phenomenon in EMDR
- Short-Term Worsening vs Long-Term Harm
- Who Is at Highest Risk for Negative Effects
- How Qualified Therapists Mitigate EMDR Risks
- EMDR in Legal Contexts The Risk to Testimony Integrity
- A Practical Guide for Clients and Attorneys
Introduction
Clients often arrive with a blunt question: can EMDR make things worse? That fear is reasonable. EMDR asks people to approach memories they've spent years avoiding, compartmentalizing, or surviving around.
The answer is nuanced. EMDR can make a person feel worse temporarily, especially when traumatic material is actively activated and processed. That isn't automatically a sign of bad treatment. In many cases, it reflects the fact that the brain is finally engaging material that had been held in a fragmented, unintegrated way.
What changes in immigration cases is the cost of getting this wrong. A transient increase in symptoms might be manageable in ordinary therapy. It becomes more consequential when a client is also preparing an affidavit, attending USCIS interviews, testifying in immigration court, or trying to preserve a coherent timeline across multiple legal documents.
Practical rule: In immigration matters, the relevant question isn't only whether EMDR helps trauma. It's whether the timing, pacing, and therapist neutrality protect both the client's stability and the integrity of their testimony.
A careful answer requires separating normal treatment activation from true clinical deterioration, and separating clinical improvement from forensic risk. Those are not the same thing.
The Before Better Phenomenon in EMDR
EMDR can temporarily intensify trauma symptoms through a documented before-better phenomenon, where the Adaptive Information Processing network activates previously isolated memory fragments. Bilateral stimulation can reactivate unprocessed traumatic neural networks, which may flood the nervous system before integration occurs, as discussed in this review of EMDR mechanisms and applications.
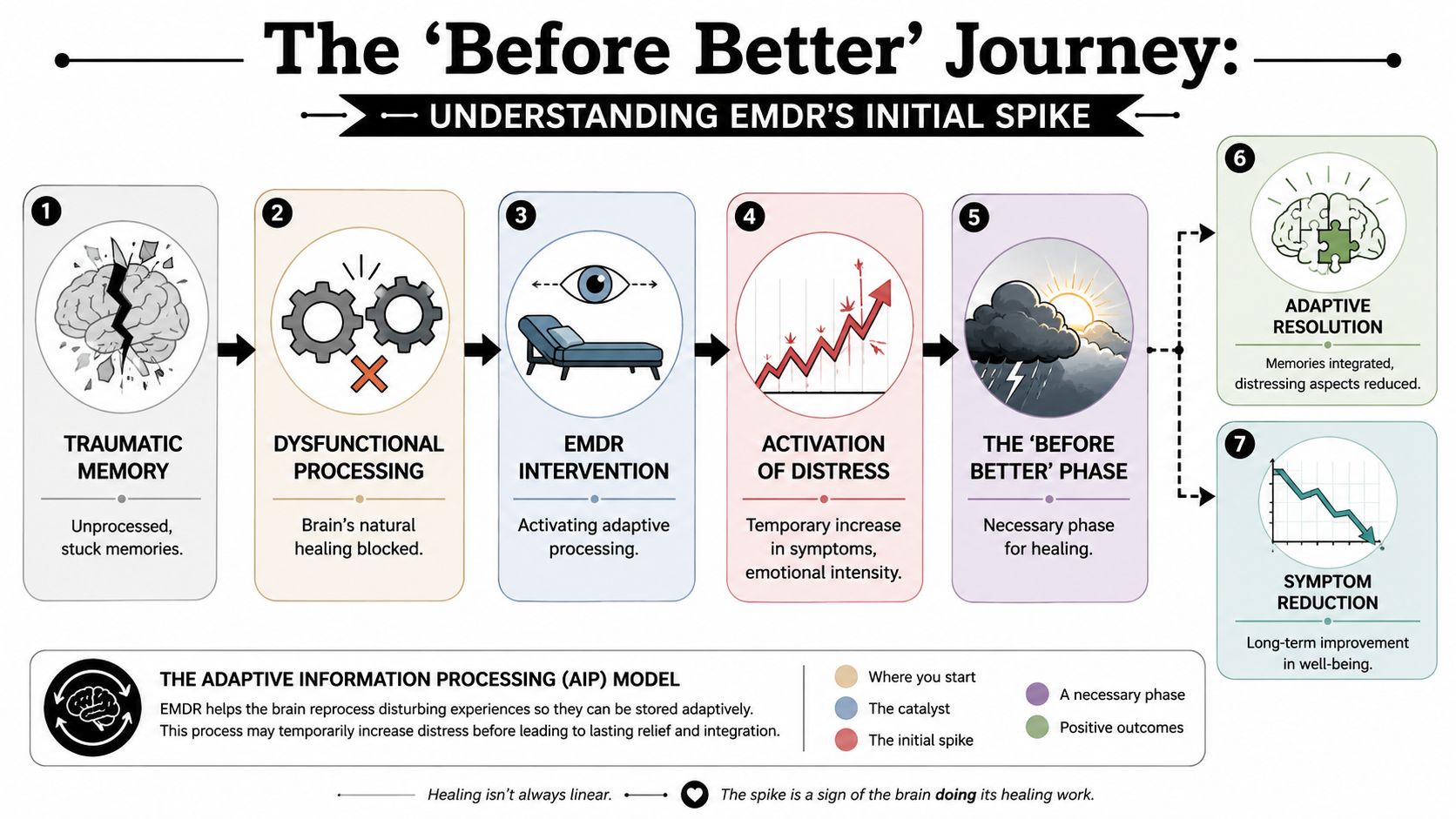
Why symptoms can spike during processing
A useful analogy is wound care. Cleaning a wound hurts. It can look worse before it looks better. But that temporary aggravation may be part of proper healing rather than evidence that the treatment itself is damaging the body.
EMDR works in a similar way. The client does not only talk about trauma in an abstract, distant way. The treatment intentionally brings up images, beliefs, emotions, and body sensations linked to the trauma so the brain can process them differently. During that activation phase, distress may rise.
That's one reason clients sometimes report increased emotional sensitivity, stronger body reactions, or more intrusive recollections between sessions. In people who already live with nervous system dysregulation, this temporary activation can feel alarming if no one explained it in advance.
What that looks like in practice
The temporary worsening often has a recognizable pattern:
- Emotional activation: A client may feel more tearful, more reactive, or more emotionally exposed after a session.
- Trauma-linked recall: Fragments of memory may return with sharper intensity before they become less disturbing.
- Body-based stress: Sleep disruption, agitation, or somatic distress can appear while the nervous system is processing loaded material.
That pattern does not mean a therapist should push forward regardless of client response. The point is narrower. Short-lived activation can occur even in appropriate treatment.
EMDR is often misunderstood when people expect symptom relief to be linear. Trauma processing rarely works that way.
For attorneys, this matters because a client who is in the middle of active reprocessing may appear more distressed, more fragmented, or less verbally organized for a period of time. That presentation can reflect active treatment rather than deception, inconsistency, or malingering. The legal team needs to know the difference.
Short-Term Worsening vs Long-Term Harm
A client can feel worse after EMDR without being harmed. In practice, the legal question is narrower. Does the treatment reaction pass, or does it begin to interfere with memory organization, daily functioning, and the client's ability to give reliable testimony?
The distinction turns on three points: how long the reaction lasts, how intense it becomes, and what it does to the person's functioning outside session. Temporary activation can be uncomfortable and still remain within the range of expected trauma work. Ongoing destabilization raises a different concern because it can alter how a client sleeps, works, parents, regulates emotion, and recounts traumatic events under pressure.
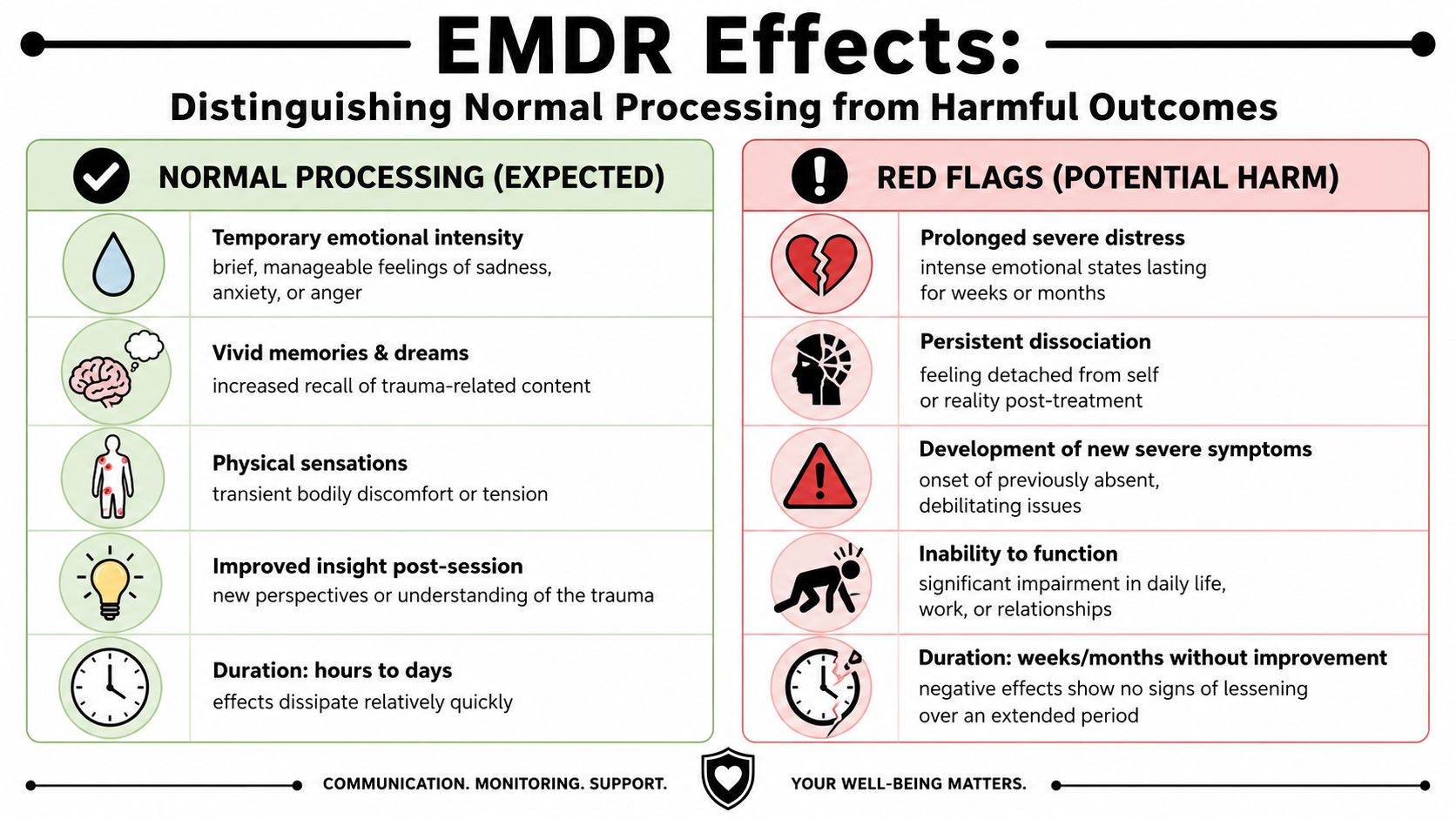
Expected processing effects
As noted earlier, EMDR follows a structured protocol and can produce temporary increases in distress between sessions. That often presents as a brief flare in symptoms rather than evidence that treatment is causing lasting damage.
| Expected short-term effects | Why they happen |
|---|---|
| Temporary emotional intensity | The memory has been activated and is no longer being held at a distance |
| Vivid dreams or stronger recall | Processing may continue between sessions |
| Fatigue or light-headedness | Trauma work places cognitive and physiological strain on the client |
| Brief increase in distress | Contact with painful material can temporarily raise arousal |
A short educational video can help clients and counsel understand that distinction before treatment begins.
Short-term worsening usually has limits. The client can still orient to the present, use grounding skills, and return to baseline within a reasonable period. Their account may be emotional, but it remains recognizable and substantially consistent.
Red flags that suggest actual harm
The concern changes when the reaction becomes prolonged, disorganizing, or difficult to contain. In forensic work, I pay close attention when treatment appears to reduce a client's capacity to stay coherent about the same core events across settings.
Warning signs include:
- Persistent dissociation: The client stays detached, unreal, foggy, or cognitively fragmented well after the session ends.
- Loss of daily functioning: Sleep, work, childcare, hygiene, or basic routines decline in a sustained way.
- Flooding that does not settle: Grounding, pacing changes, or ordinary stabilization do not bring the client back within their window of tolerance.
- Growing narrative instability: Recall becomes more confused, more suggestible, or less anchored to previously stable facts.
Clinical caution: Temporary activation can be expected. Persistent destabilization requires reassessment.
For immigration cases, that distinction matters immediately. A brief increase in distress may have little legal significance if the client remains oriented and consistent. A prolonged period of dissociation, disorganization, or unstable recall can create avoidable problems for affidavits, credible fear interviews, merits hearings, and cross-examination.
Attorneys do not need to assume bad faith when a client looks more distressed during active trauma treatment. They do need to ask whether the treatment is helping the client process traumatic material or impairing the client's ability to recount it clearly. If the answer is the latter, the treatment plan may need to be paused, slowed, or changed.
Who Is at Highest Risk for Negative Effects
Risk isn't evenly distributed. The better question is not merely whether EMDR can worsen symptoms. It's how clinicians decide when the risk is high enough to stabilize first.
That question is especially important for clients with complex trauma histories or pre-existing dissociative symptoms, as emphasized in this clinical discussion of EMDR risk factors and stabilization needs.
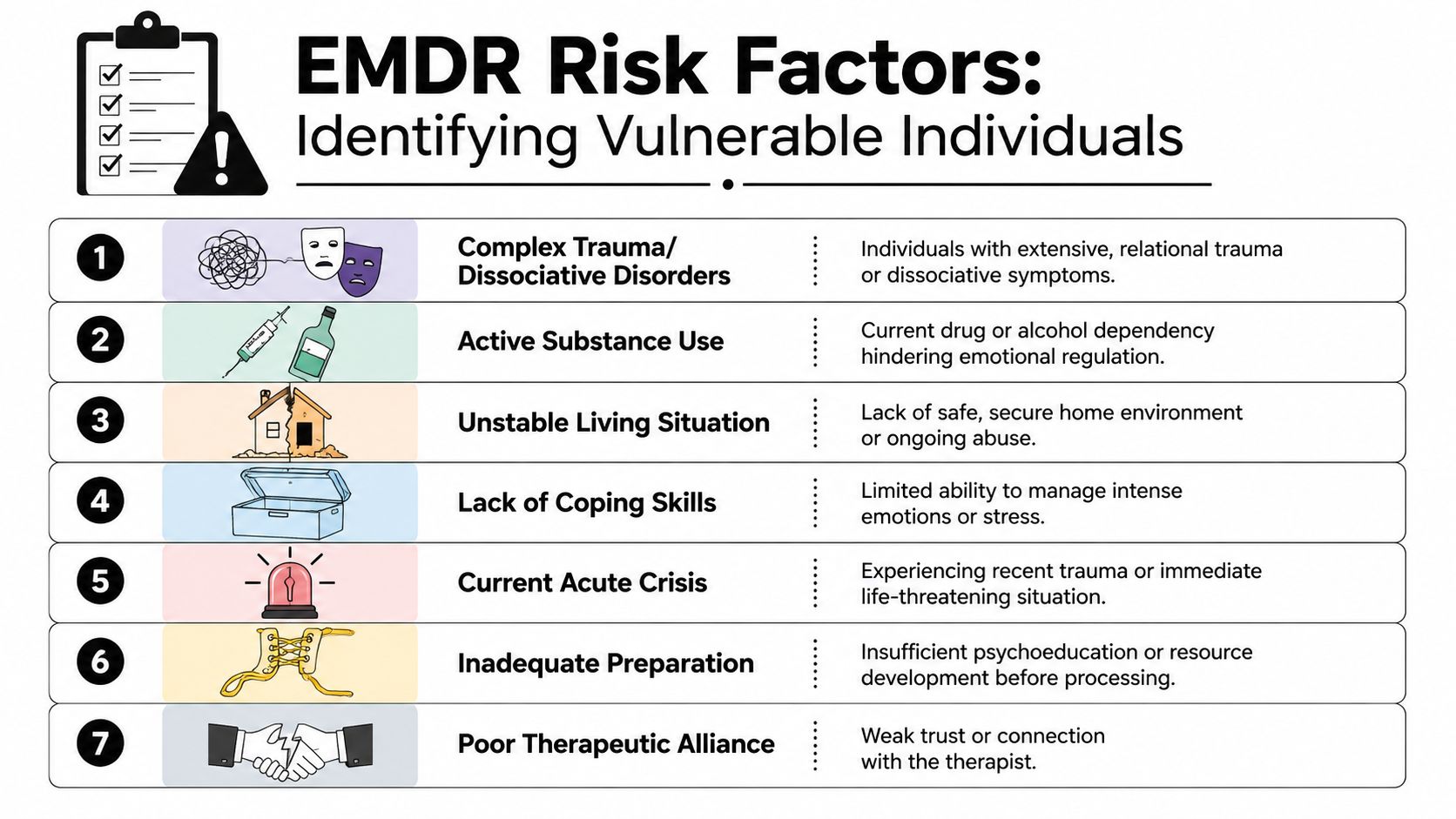
The clients who need slower pacing
In forensic and immigration settings, the highest-risk group often includes people whose trauma was chronic, relational, and repeated. They may have learned to survive through fragmentation, numbing, compartmentalization, or rapid shifts in state. Standard trauma processing can exceed their current capacity if the therapist moves too fast.
Examples include:
- Complex trauma and dissociation: These clients may lose time, detach from the present, or struggle to stay anchored while trauma material is activated.
- Acute instability: Ongoing danger, housing insecurity, active abuse, or crisis conditions can make intensive trauma processing poorly timed.
- Weak coping capacity: Some clients have never been taught grounding, affect regulation, or containment strategies.
- Fragile therapeutic alliance: If trust is thin, clients may comply outwardly while becoming internally overwhelmed.
Why this matters in immigration cases
Immigration clients often carry several of these risk factors at once. A trafficking survivor may still fear retaliation. An asylum applicant may be living in precarious housing. A domestic violence survivor may be safe from the perpetrator but not yet emotionally stable enough for direct reprocessing.
That doesn't mean EMDR is contraindicated forever. It means stabilization may need to come first.
Here is the practical legal relevance:
- Declaration drafting can be affected: A client who enters treatment too early may become less organized while preparing a statement.
- Interview readiness can drop: A person may know what happened but struggle to narrate it coherently during an active destabilization period.
- Credibility concerns can intensify: Trauma-related fragmentation may be misread by adjudicators if the legal team doesn't understand the clinical context.
A cautious therapist who delays trauma processing is not avoiding treatment. In many cases, that clinician is protecting the client from becoming clinically and legally more vulnerable.
Attorneys should hear “we need stabilization first” as a mark of competence, not hesitation. In high-stakes cases, restraint is often the safer choice.
How Qualified Therapists Mitigate EMDR Risks
EMDR is not just eye movements. It is a structured, multi-phase treatment, and safety depends heavily on whether the therapist uses that structure properly.
A 2025 systematic review reported that a third of the included studies had a 0% dropout rate in the EMDR condition, while waitlist controls had a 15.58% dropout rate, supporting the view that most participants completed treatment and that serious worsening is uncommon when the protocol is followed, according to the systematic review in Scandinavian Journal of Psychology.
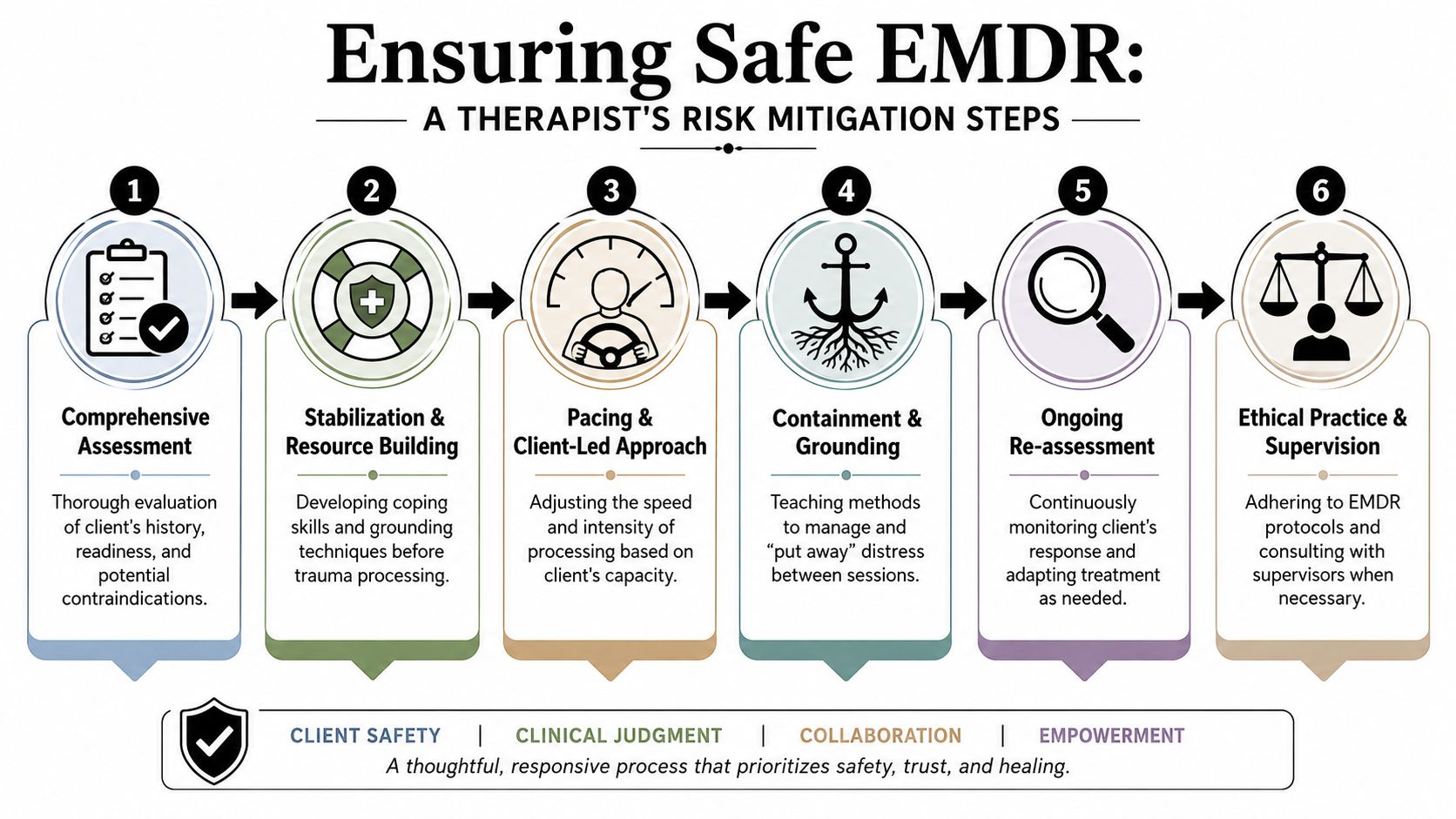
What competent risk management actually looks like
A qualified therapist doesn't start with the most disturbing memory on day one. They assess readiness, teach regulation skills, and monitor whether the client can tolerate activation without losing stability.
That is especially important with clients who have complex PTSD and EMDR treatment considerations, where standard pacing may be too aggressive.
Key safeguards include:
Screening before processing
The therapist looks for dissociation, severe instability, psychotic symptoms, or other signs that direct trauma work may need to wait.Preparation and resourcing
Clients learn grounding, containment, and emotion-regulation methods before processing begins.Pacing the work
The therapist adjusts intensity based on client response, not on a rigid agenda.Stopping when needed
Good EMDR includes the ability to pause, shift, or return to stabilization if the client becomes overwhelmed.
What doesn't work
Some failures are predictable. Problems arise when a clinician treats EMDR like a fast-track exposure tool, rushes into target memories, or assumes distress automatically means progress.
That approach is risky in any setting, but especially risky for clients involved in legal proceedings.
A poor process often includes:
- Minimal assessment: The therapist doesn't meaningfully screen for dissociation or instability.
- Thin preparation: The client enters processing without reliable self-soothing tools.
- Suggestive guidance: The therapist steers meaning or memory content instead of remaining neutral.
- No coordination with timing demands: Treatment begins without regard to upcoming declarations, hearings, or interviews.
The strongest protection against EMDR-related harm is not the modality alone. It's the clinician's discipline in using the modality correctly.
For attorneys, therapist selection matters as much as treatment selection. The wrong therapist can create avoidable problems even with a legitimate method.
EMDR in Legal Contexts The Risk to Testimony Integrity
The central forensic issue is not whether EMDR reduces distress. It often does. The issue is whether the treatment could alter how memory is expressed in a case where detail, sequence, and internal consistency matter.
EMDR carries a specific risk of memory distortion or false memory formation. The concern is that memory reconsolidation during bilateral stimulation can alter original encoding, creating a significant liability when legal proceedings depend on evidentiary consistency, as discussed in this analysis of EMDR, memory, and courtroom risk.
Why the legal risk is different from the clinical risk
In ordinary treatment, a slight shift in how a client experiences a memory may not be catastrophic if the person becomes less symptomatic and more functional. In immigration law, the standards are different. The client may need to recount abuse, persecution, trafficking, or coercion across affidavits, intake notes, declarations, interviews, and testimony.
Even a clinically understandable change can create problems if it appears as:
- a newly emerging detail that cannot be corroborated,
- a contradiction with earlier statements,
- confusion about sequence,
- stronger confidence in a memory fragment that remains uncertain.
That does not mean EMDR is improper for all immigration clients. It means the forensic stakes are higher, so treatment decisions need more planning.
Therapist neutrality is not optional
The risk of memory distortion grows when the therapist is suggestive, interpretive, or invested in uncovering hidden material. In legal cases, neutrality matters. A therapist should not guide a client toward a preferred narrative or treat emerging imagery as verified fact.
Attorneys should be alert to language in records that implies interpretation rather than observation. Notes should distinguish clearly between what the client reported, what the client remembered with uncertainty, and what arose during processing without external verification.
If a client's legal case depends on precise testimony, the safest therapeutic stance is careful, neutral, and non-interpretive.
Practical implications for case strategy
There are times when EMDR may still be appropriate during a pending case. There are also times when a more supportive or stabilization-based approach is wiser until major testimony is complete.
A practical framework for attorneys is this:
- If testimony is imminent, be cautious about starting intensive reprocessing.
- If the client already shows dissociation or confusion, prioritize stability over rapid trauma processing.
- If treatment is underway, document the type of treatment and any period of temporary activation that could affect presentation.
- If recall becomes more contradictory after EMDR, address that issue early rather than hoping it won't matter.
The legal system tends to reward coherence. Trauma treatment sometimes temporarily disrupts coherence before helping restore it. That tension has to be managed deliberately.
A Practical Guide for Clients and Attorneys
The safest way to approach EMDR in an immigration matter is not to ask whether the treatment is good or bad in the abstract. Ask whether it is appropriate for this client, at this time, with this therapist, in this legal posture.
Questions clients should ask before starting EMDR
A client doesn't need technical expertise. They do need a therapist who can answer direct safety questions clearly.
Useful questions include:
How do you decide whether someone is ready for EMDR?
The answer should include assessment of stability, coping skills, and dissociation risk.What do you do before trauma processing begins?
Listen for grounding, preparation, resourcing, and a plan for between-session distress.How do you handle overwhelm or dissociation during a session?
A good therapist should describe how they slow down, pause, and re-stabilize.How do you avoid influencing memory?
The answer should emphasize neutrality rather than interpretation.How will I know if a reaction is expected or a sign we should stop?
Clients need concrete guidance, not reassurance alone.
Questions attorneys should ask when treatment overlaps with a case
Attorneys do not need to direct therapy. They do need enough information to protect the case and the client.
Consider asking, with proper releases in place:
| Attorney concern | Practical question |
|---|---|
| Timing | Is this a period of stabilization or active trauma reprocessing? |
| Functional impact | Is treatment likely to temporarily affect concentration, sleep, or emotional regulation? |
| Testimony integrity | Are there concerns about confusion, dissociation, or shifting recall? |
| Case planning | Would it be wiser to defer intensive processing until after major testimony? |
A sound default approach
For many immigration clients, the safest sequence is simple:
- Stabilize first: Build regulation, safety, and predictability.
- Coordinate timing: Don't ignore interview dates, affidavit deadlines, or hearing prep.
- Document carefully: If treatment affects presentation, that context may matter later.
- Stay flexible: If EMDR is destabilizing, pause and shift rather than forcing continuation.
Clients need relief. Attorneys need reliable narratives. Good clinical care can support both, but only when the treatment plan respects the legal reality around the case.
If your case requires a trauma-informed psychological evaluation that addresses symptom presentation, credibility-related clinical issues, and the forensic implications of treatment history, Pro Psychological Analysis provides immigration-focused assessments for attorneys handling asylum, VAWA, T visa, U visa, and hardship matters.