You're often handed a stack of records at the worst possible moment. The declaration is nearly done. Filing deadlines are close. The client has treatment notes, a discharge summary, a few emergency room pages, maybe a therapist letter, and all of it feels important. Yet when you read it as an immigration attorney, the record doesn't adequately answer the question USCIS or the immigration court will care about.
That gap is where many cases weaken. The client may be telling the truth. The harm may be real. The symptoms may be significant. But medical documentation only becomes persuasive legal evidence when it is organized, attributable, time-stamped, and tied to the precise issue the adjudicator must decide.
In immigration practice, that distinction matters more than many clinicians realize. A treatment chart can help explain what happened in care. A forensic evaluation can do something different. It can translate history, symptoms, observations, and records into a structured opinion that supports a legal theory without slipping into advocacy disguised as medicine.
Table of Contents
- More Than a File A Strategic Asset in Immigration Law
- Defining Medical Documentation Beyond the Clinic
- Key Types of Medical Evidence in Immigration Cases
- The Critical Role of Documentation in Specific Claims
- Meeting Admissibility and Evidentiary Standards
- Anatomy of a Strong Clinical Report for USCIS
- Navigating Confidentiality HIPAA and Ethical Duties
- Frequently Asked Questions About Medical Documentation
More Than a File A Strategic Asset in Immigration Law
An attorney receives clinic notes for an asylum case. The pages show insomnia, headaches, panic, missed work, and a history of trauma. On paper, that sounds useful. In practice, the record is thin. Dates are inconsistent. The writer's role isn't clear. Symptoms are listed, but the notes never explain how the clinician connected those symptoms to the reported persecution, or whether the clinician considered other explanations.
That kind of record isn't worthless. It wasn't built for the legal burden you're trying to meet.
A strong immigration filing needs more than proof that a client sought care. It needs documentation with forensic value. That means the record does more than describe distress. It identifies who evaluated the client, when they did it, what information they reviewed, what they observed, and how they reached their conclusions.
Practical rule: A document becomes strategically useful when an adjudicator can follow the path from facts to opinion without guessing.
In immigration cases, medical documentation often carries two jobs at once. First, it preserves a clinical history. Second, it gives the legal team a disciplined way to present injury, trauma, impairment, fear, abuse dynamics, or hardship in language that fits evidentiary review.
That's why a purpose-built psychological evaluation can become central rather than supplemental. It can help establish consistency, explain delayed disclosure, document trauma sequelae, distinguish memory fragmentation from fabrication, and connect symptoms to the immigration claim in a way ordinary treatment records usually don't.
Attorneys who treat medical evidence as a last-minute attachment often end up with records that are reactive and incomplete. Attorneys who treat it as part of case strategy usually get something far more valuable: a report that supports declarations, prepares clients for testimony, and gives USCIS or the court a coherent factual and clinical narrative to evaluate.
Defining Medical Documentation Beyond the Clinic
What is medical documentation? In the strict sense, it is the written or electronic record used to track a patient's condition and communicate clinical decisions. Widely accepted standards require core elements such as patient identification on each page, dated entries, author identification, and clear problem lists. The American College of Physicians discussion of documentation standards also notes that NCQA identifies 6 core elements among 21 commonly accepted standards in medical record documentation, underscoring that the record is meant to be structured and auditable, not casual note-taking (American College of Physicians overview of documentation standards).
The clinical record and the legal record are related but not identical
In a clinic, documentation supports treatment, communication, follow-up, and continuity of care. In a legal setting, the same record may be read for a different purpose. The adjudicator wants to know whether the information is reliable, whether it was recorded in a methodical way, and whether the author's conclusion rests on identified facts rather than assumption.
That's why attorneys benefit from separating assessment from evaluation. Assessment gathers the material. It includes interviews, observations, symptoms, prior records, and test results when available. Evaluation answers the central question. It interprets the material in relation to the case.
If you want a useful parallel, compare it to the difference between intake and analysis. Or, in psychological terms, compare raw data to a formulated opinion. This is also the distinction many readers miss when they read broad explanations of what a clinical assessment involves.
Think of it as a detective file
The best working analogy is a detective file. A detective doesn't just collect scraps of information. The detective organizes statements, dates, corroboration, observations, and inconsistencies so another person can review the file and understand why a conclusion was reached.
Medical documentation operates the same way when it is prepared for immigration use. The strongest records do several things at once:
- Identify the source clearly. The reader should know who wrote the record and in what role.
- Anchor the timeline. Dates matter. A note without a date loses force quickly.
- Separate facts from interpretation. Reported symptoms, observed behavior, and clinical opinion should not blur together.
- Preserve reasoning. The record should show why the clinician reached the diagnosis or formulation.
- Support review by third parties. A useful record can be read by USCIS, counsel, opposing counsel, or a judge without requiring the clinician to fill in major gaps later.
Good documentation doesn't just say what happened. It shows how the clinician knows what they're saying.
For immigration counsel, that shift in perspective changes how you request evidence. You're not just asking, “Does the client have records?” You're asking whether the record can withstand legal reading.
Key Types of Medical Evidence in Immigration Cases
Not all medical evidence does the same work. Attorneys usually see three broad categories, and each has a different level of strategic value.
Treating records
Treatment records come from ongoing care. These may include primary care notes, hospital records, psychiatry visits, therapy charts, medication management entries, or emergency department paperwork. Their strength is that they often show contemporaneous care. They can document symptoms, diagnoses, medications, referrals, crisis episodes, and functional difficulty close in time to the events at issue.
Their weakness is equally important. Most treating clinicians are documenting for care, not for adjudication. They may not ask the questions needed for an asylum nexus analysis. They may not explore abuse dynamics in a VAWA matter. They may not describe hardship in a way that maps neatly onto a waiver argument.
Forensic psychological evaluations
A forensic psychological evaluation is different because it is built around the legal question. The evaluator gathers history, reviews available records, documents symptoms and functioning, and then explains how the findings relate to the case theory. That structure gives the report more evidentiary weight when the issue is not solely whether treatment occurred, but what the documented condition means for the claim.
For lawyers who handle more medically complex matters, it can help to understand how a deeper comprehensive neuropsychological evaluation differs from a shorter clinical opinion. The same general principle applies across forensic work. The more clearly the method fits the question, the more useful the final report becomes.
Brief letters and summary notes
Short letters from therapists, social workers, or physicians often appear in filings because they are easier to obtain. Sometimes they help. A concise note can confirm treatment dates, diagnosis, observed symptoms, or the provider's role.
But these letters frequently underperform for one simple reason. They summarize conclusions without documenting the underlying method. If the letter says the client has trauma symptoms but doesn't describe the interview basis, review of records, observations, and reasoning, the attorney is left with an assertion that may be sympathetic but not especially durable.
A quick comparison helps:
| Evidence type | Usually strongest for | Common weakness |
|---|---|---|
| Treating records | Showing care history and symptom chronology | May not address the legal issue directly |
| Forensic evaluation | Linking clinical findings to the immigration claim | Requires more planning and coordination |
| Brief provider letter | Confirming diagnosis or treatment status | Often lacks detailed reasoning and forensic structure |
The practical point is simple. Use each form of evidence for what it does well. Don't ask a treatment note to perform the work of a forensic report.
The Critical Role of Documentation in Specific Claims
The same symptom can matter differently depending on the claim. Panic attacks in an asylum case are not doing the same evidentiary work as panic attacks in a hardship waiver. Good documentation changes with the legal target.
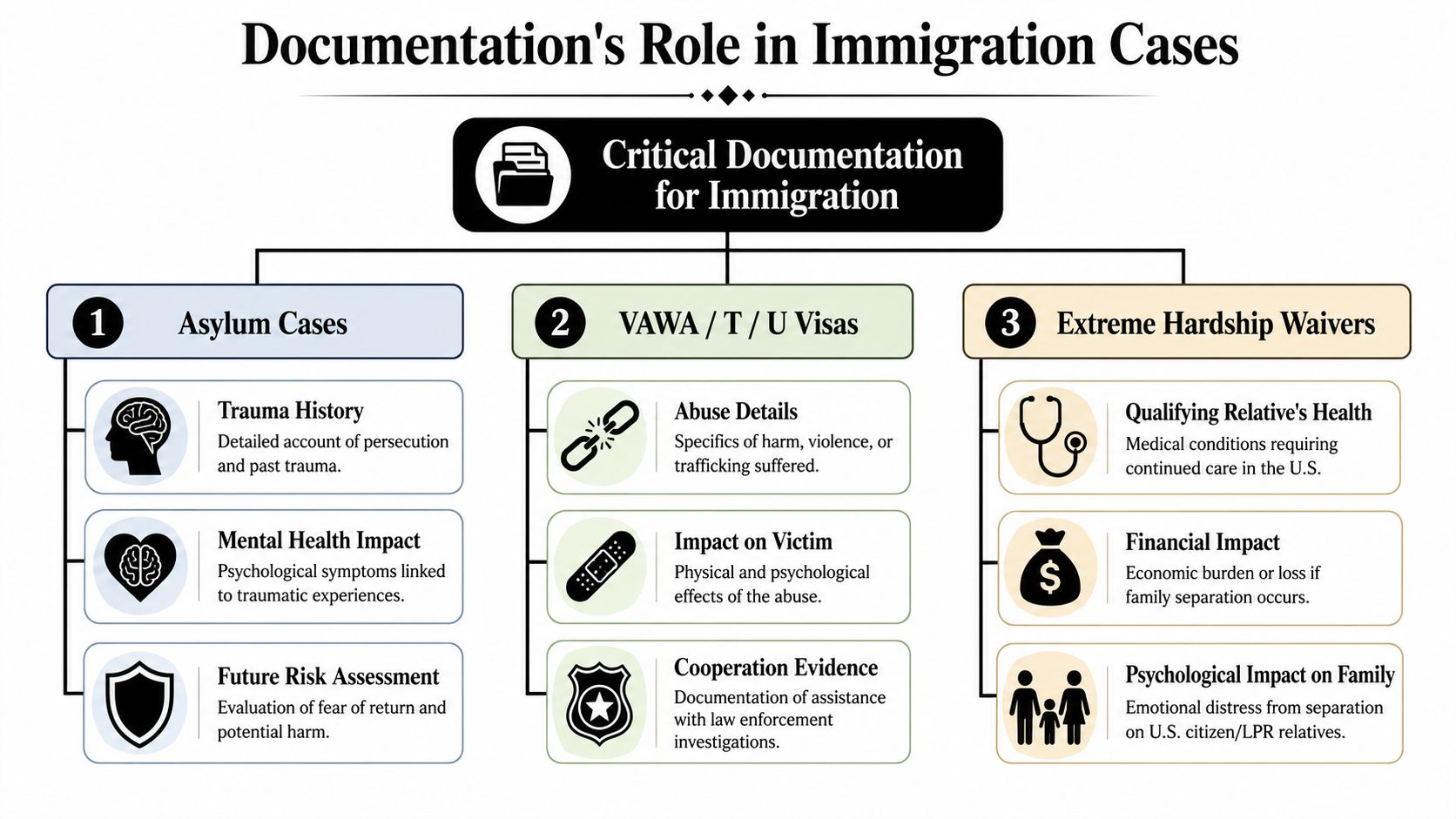
Asylum claims
In asylum matters, documentation often helps establish the psychological impact of persecution, torture, threats, detention, sexual violence, or other traumatic exposure. The key is not merely proving that the client is distressed. It is showing that the distress is clinically coherent, consistent with the reported history, and relevant to fear, past harm, memory fragmentation, avoidance, or delayed disclosure.
A strong evaluation can clarify several issues that routinely arise in asylum cases:
- Trauma narrative coherence. Traumatized clients often recount events in fragments. A careful report can explain why.
- Symptom linkage. The clinician should connect reported symptoms to the traumatic experiences with clear reasoning.
- Functional impact. Sleep disruption, hypervigilance, dissociation, concentration problems, and social withdrawal often matter because they affect credibility presentation and day-to-day functioning.
- Future risk framing. Where appropriate, documentation can explain why return may worsen symptoms or recreate trauma-related responses.
VAWA T and U matters
Cases involving domestic violence, trafficking, coercion, or qualifying criminal victimization require a different lens. The record should address abuse dynamics, not just injuries. That means coercive control, fear conditioning, trauma bonding, dependence, threats to children, threats related to immigration status, and the psychological reasons a victim may have stayed, delayed reporting, or returned to the perpetrator.
Those issues matter because legal decision-makers sometimes read behavior through a common-sense lens that doesn't fit trauma reality.
A clinically useful report in victim-based immigration cases often explains behavior that a non-clinician might otherwise misread as inconsistency.
In these matters, attorneys often benefit from pairing the evaluation with a carefully framed hardship narrative, especially when family impact overlaps with the victim's own trauma history. That overlap is one reason many lawyers also refine their evidentiary strategy around how to write a letter of hardship.
Extreme hardship waivers
Hardship cases require discipline because broad claims of sadness, disruption, or stress usually aren't enough. The documentation must focus on the qualifying relative and explain why separation or relocation would create hardship that is medically or psychologically substantial.
What helps most is specificity. If a qualifying relative has an existing medical condition, the record should describe treatment needs, care continuity issues, medication management, psychiatric vulnerability, caregiving demands, and the likely impact of separation on stability and functioning. If the hardship is primarily psychological, the evaluator should document baseline functioning, current symptoms, precipitating stressors, and why the immigration outcome materially changes the clinical picture.
Weak hardship evidence says the family will suffer. Strong hardship evidence shows who will suffer, how, and why the expected impact is clinically serious.
Meeting Admissibility and Evidentiary Standards
A report doesn't become persuasive because it uses diagnostic language. It becomes persuasive because the evaluator documents the path from data to conclusion.
Why the reasoning matters as much as the diagnosis
A legally strong medical record should document the clinical reasoning pathway, not just the endpoint. Guidance in the NIH-hosted review emphasizes recording the risk-benefit analysis behind decisions, the clinician's judgment at key points, and transparent entries that support record integrity and later review (NIH review on legal strength and clinical reasoning in medical records).
For immigration work, that principle has enormous practical value. If an evaluator concludes that a client meets criteria for a trauma-related condition, the report should show what facts support that conclusion. What symptoms were reported? What was observed? What prior records were reviewed? What alternatives were considered? Why does the diagnosis fit better than another explanation?
That level of structure matters because USCIS and immigration courts do not only read for compassion. They are reading for reliability. A report that lays out method, factual basis, and reasoning gives the adjudicator something they can trust.
What weakens a report under scrutiny
Attorneys usually see the same problems repeatedly. The diagnosis appears in the first paragraph, but the body of the report never explains it. The clinician repeats the client's narrative in detail, yet offers almost no independent observations. Records are mentioned vaguely without identifying what was reviewed. Dates don't line up. Translation issues are ignored. The report reads like advocacy copy rather than disciplined clinical analysis.
A strong report avoids those traps. It distinguishes between what the client said, what the clinician observed, and what the clinician inferred. It also stays inside the evaluator's role. A clinician may support facts relevant to the case, but shouldn't act as if they are deciding the legal outcome.
Consider this quick contrast:
- Less persuasive: “The client is credible and deserves relief.”
- More persuasive: “The client's symptom presentation, affective response, and reported trauma history were clinically consistent with the type of traumatic exposure described.”
That difference sounds subtle. In practice, it is not. One statement reaches beyond the clinician's lane. The other gives the attorney and adjudicator usable material without overclaiming.
Anatomy of a Strong Clinical Report for USCIS
Attorneys don't need to become clinicians, but they do need a practical sense of what a complete report should contain. When the structure is missing, the filing usually shows it.
Core sections that should be there
High-quality documentation should be complete, accurate, and time-stamped, and it should capture objective evidence while clearly separating that material from patient-reported symptoms because objective findings are more reproducible and more defensible in audit and legal review (TechTarget definition of clinical documentation and why objective evidence matters). In an immigration evaluation, that principle translates into a report with recognizable forensic parts.
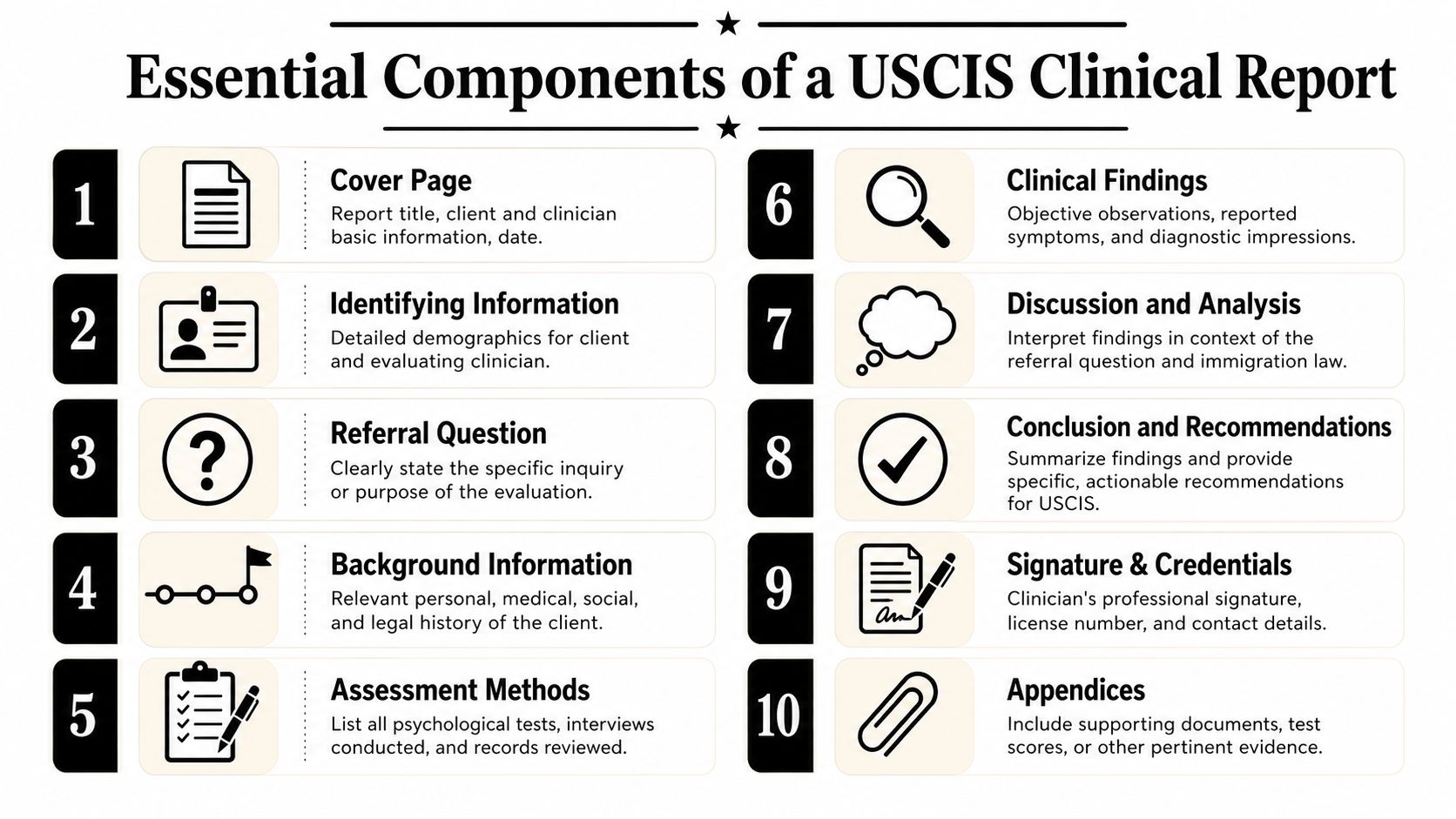
A strong report usually includes:
- Identifying information. Who was evaluated, by whom, on what date, and for what immigration purpose.
- Referral question. The exact issue the evaluation is meant to address.
- Sources of information. Interviews, collateral records, prior treatment notes, declarations, and other reviewed materials.
- Relevant background. Social, developmental, medical, psychiatric, family, occupational, and trauma history, limited to what is clinically and legally relevant.
- Mental status or behavioral observations. What the evaluator directly observed during the interview.
- Diagnostic impressions or formulation. The clinical conclusions and the reasoning supporting them.
- Functional analysis. How symptoms affect sleep, work, caregiving, memory, concentration, daily activities, or safety.
- Case-specific opinion. The section that connects findings to the immigration issue without drifting into legal argument disguised as diagnosis.
- Signature and credentials. The report must be attributable to a licensed professional with identifiable qualifications.
What attorneys should check before filing
When I review reports for legal use, I look first for integrity, not flourish. The report should read cleanly enough that another professional could understand the path of the evaluation.
Review test: If you removed the diagnosis line, would the rest of the report still lead a careful reader to the same conclusion?
Use this short filing screen before attaching a report:
- Dates and authorship are clear. Every major document should be attributable.
- The evaluator identified the materials reviewed. Vague references to “records” aren't enough.
- Observed facts and reported facts are separated. This protects credibility.
- The formulation answers the legal need. Not in legal jargon, but in clinically relevant terms.
- The tone is measured. Strong reports are confident without sounding promotional.
When those elements are present, the report helps the attorney make an argument. When they are absent, the attorney ends up rewriting around the report's weaknesses.
Navigating Confidentiality HIPAA and Ethical Duties
Immigration clients often ask the same question in different forms: who will see this? That isn't a side issue. In trauma-related work, the answer affects disclosure, trust, and the accuracy of the history you're able to obtain.

Consent and controlled disclosure
A professionally handled immigration evaluation should begin with informed consent and a clear explanation of the evaluator's role. The client needs to understand whether the evaluation is for treatment, forensic reporting, or both. They also need to know who may receive the final report, what records are being requested, and what limits apply to confidentiality.
For attorneys, this is not just risk management. Ethical clarity improves the quality of the evidence. Clients disclose more accurately when they know the boundaries. Evaluators write more carefully when the audience and purpose are explicit.
That process usually includes a release of information. The release should identify what can be disclosed, to whom, and for what purpose. It should not be treated as a casual administrative form.
Digital records and ethical handling
The move from paper to digital systems has made recordkeeping more auditable and more operationally complex. The HHS Office of Inspector General states that proper documentation protects patients, programs, and providers, and one industry report cited in that discussion projected the ambient clinical documentation market at $600 million in 2025 after major growth; the same report noted physicians using AI tools spent 64.76% less time on paperwork (HHS OIG discussion of why documentation matters and the trend toward auditable digital workflows). Those figures are about healthcare operations, but they point to the same reality immigration practitioners now face. Records are increasingly electronic, searchable, shareable, and reviewable.
That creates trade-offs. Digital systems improve legibility and tracking. They also make copy-forward errors, metadata issues, and over-disclosure easier if the workflow is sloppy.
A careful practice should account for:
- Minimum necessary sharing. Send what the case needs, not every page available.
- Interpreter documentation. If language access shaped the interview, the record should reflect that.
- Correction transparency. If a note is corrected, the correction should be attributable and clear.
- Secure transfer. Convenience should not outrun privacy.
A brief overview can help clients understand why these rules exist and why providers take them seriously:
A report that reflects ethical discipline tends to read as more credible. The opposite is also true. If consent is muddy, disclosure is excessive, or the evaluator's role is unclear, those flaws don't stay hidden. They show up in the document.
Frequently Asked Questions About Medical Documentation
For attorneys
How do I handle inconsistencies between testimony and the medical record?
Treat the inconsistency as a problem to analyze, not a flaw to bury. First determine what kind of inconsistency it is. Date confusion, trauma-related fragmentation, translation error, and genuine contradiction are not the same thing. If the issue is material, ask for clarification before filing and make sure any evaluator has the updated facts.
When is an updated evaluation worth obtaining?
Usually when the client's condition has changed, the case posture has changed, the original report is outdated for your litigation needs, or the earlier report didn't address the legal question cleanly enough. An update can also help when treatment records developed after the first evaluation materially deepen the picture.
Can a brief treatment letter be enough?
Sometimes, but only for narrow purposes. It may confirm treatment, diagnosis, or care continuity. It usually won't do the heavier work of forensic analysis.
Should I worry if the report is sympathetic in tone?
Sympathy isn't the problem. Overreach is. A report should be humane and clinically grounded, but it should not read like closing argument.
For clients
What if I have trouble talking about my trauma?
That is common. Trauma often affects memory, sequencing, concentration, and emotional tolerance. A competent evaluator should pace the interview carefully and document the limits as part of the clinical picture rather than treating difficulty speaking as a lack of truthfulness.
Will my medical information be shared with anyone else?
Only according to the permissions you authorize and the professional rules governing the evaluation. Ask who will receive the report, whether your attorney will control distribution, and whether any collateral records will be requested.
Do I need every medical record I've ever had?
Usually not. More paper doesn't automatically create stronger evidence. Relevant, organized records are better than a large but unfocused file.
What if I never got treatment after the harm happened?
Lack of treatment does not erase trauma. Many survivors don't seek care immediately because of fear, access barriers, stigma, language concerns, or instability. A forensic evaluation can still document current symptoms and explain clinically relevant reasons for delayed care.
The strongest immigration documentation is not the thickest file. It is the record that answers the right question with discipline.
Can a medical report guarantee approval?
No. Medical evidence is one part of the case. It can strengthen facts, explain behavior, and support legal arguments, but it doesn't replace testimony, declarations, corroboration, or legal briefing.
If your firm needs immigration-focused psychological evidence that is methodical, clear, and built for legal review, Pro Psychological Analysis works with attorneys nationwide to produce forensic evaluations for asylum, VAWA, T visa, U visa, and extreme hardship matters. Their reports are structured to translate clinical findings into persuasive legal support while maintaining strict confidentiality and ethical rigor.