You finish a client interview, close the file, and move to the next task. But the testimony doesn't stay in the room. It follows you into email triage, into the drive home, into dinner, and sometimes into sleep. If you work in immigration law, especially with asylum, VAWA, T, or U matters, that lingering effect isn't unusual. It's an occupational exposure.
Legal advocates often assume the problem is stress, overwork, or lack of resilience. Sometimes it is. But repeated exposure to detailed trauma narratives can produce a different pattern. The symptoms may affect attention, judgment, boundaries, sleep, and even how you interpret risk, credibility, and safety. That has consequences for both case quality and career longevity.
For law firms handling trauma-heavy caseloads, recognizing vicarious trauma symptoms is part of competent practice. It helps you identify when a professional needs support, when a workflow problem needs correction, and when a case team is at risk of drifting into avoidant or over-identified advocacy.
Table of Contents
- The Hidden Cost of Advocacy
- Defining Vicarious Trauma Beyond the Buzzword
- Recognizing the Key Symptom Clusters
- Is It Trauma Burnout or Secondary Stress
- How Symptoms Translate to Evidence in Immigration Cases
- Sustainable Advocacy and Professional Self-Care
- Building a Trauma-Informed Practice
The Hidden Cost of Advocacy
Immigration practice asks professionals to do something psychologically demanding. You must listen with precision, establish trust quickly, absorb disturbing facts, and convert suffering into legally useful evidence. That combination creates risk.
Vicarious trauma has been recognized for decades as a measurable occupational hazard in helping professions. The concept was first identified in the 1980s as the “cost of caring,” and by the mid-1990s it was recognized as a distinct trauma-related response linked to repeated exposure to others' traumatic experiences, including work in legal advocacy settings, as described in the California Department of Corrections and Rehabilitation trauma fact sheet.
That history matters because it corrects a common mistake. Vicarious trauma isn't just “having a hard week.” It isn't a character flaw, and it isn't proof that someone is too empathic for this work. It's a predictable exposure effect in professions that require sustained contact with traumatic material.
What legal professionals usually notice first
The first signs are often subtle:
- Attention changes: You reread declarations and can't retain them.
- Carryover outside work: A client's account intrudes while you're with family.
- Boundary strain: You feel compelled to stay psychologically available after hours.
- Emotional blunting: You can discuss severe violence fluently, yet feel detached from ordinary life.
Those patterns matter because they affect performance before anyone names the problem. Missed details, avoidant drafting, irritability with staff, and overreaction to routine case setbacks all have downstream effects.
Practical rule: If trauma-heavy work is changing how you sleep, relate, concentrate, or assess safety, treat it as an occupational health issue, not a private weakness.
In legal settings, the stakes are unusually high. A compromised advocate may still look productive. They may bill, appear composed, and meet deadlines while subtly losing flexibility, empathy, and judgment. That's why symptom recognition belongs inside supervision, not just inside personal coping.
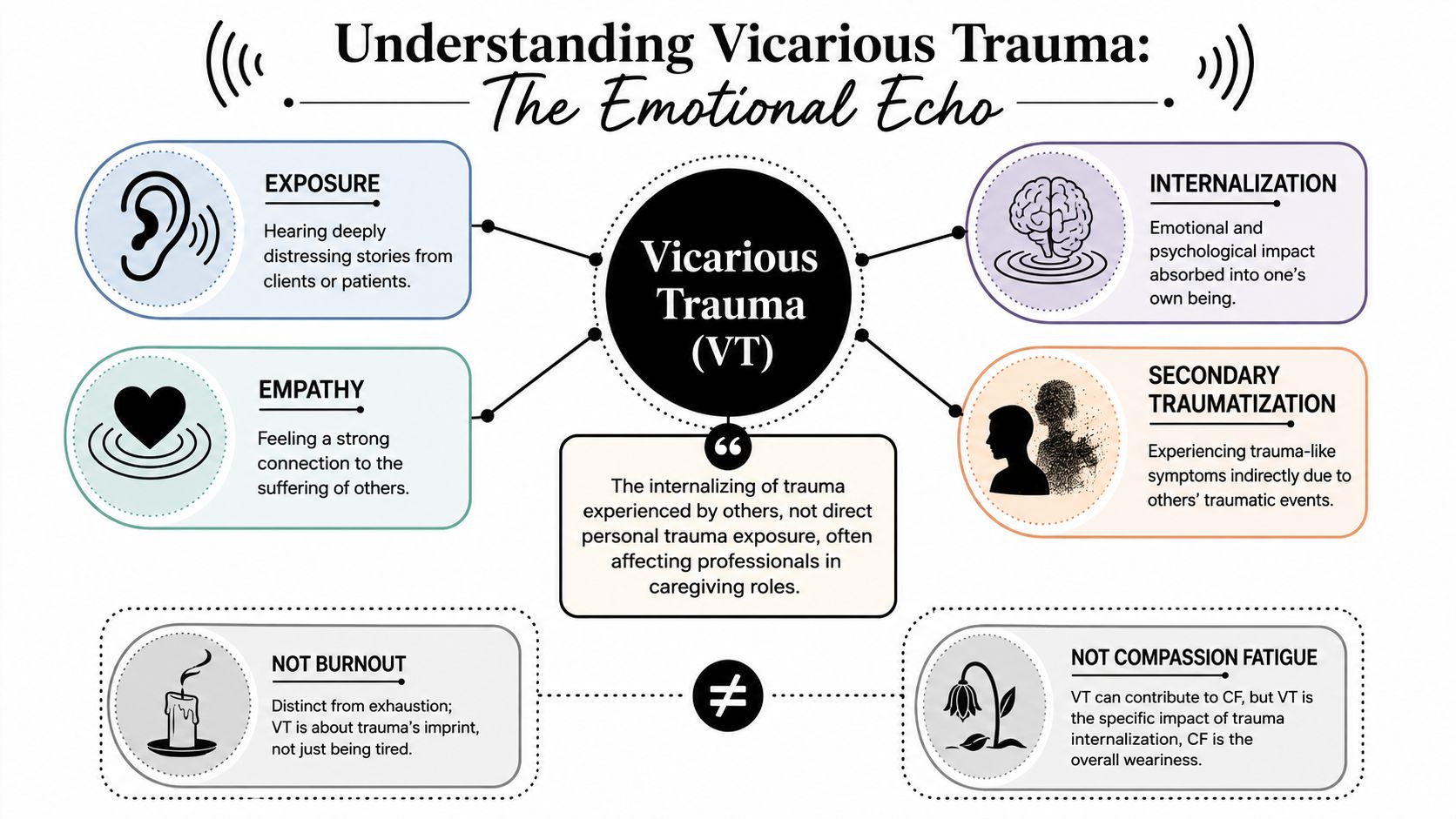
Defining Vicarious Trauma Beyond the Buzzword
Think of vicarious trauma as emotional residue with cognitive consequences. A single difficult interview may leave distress behind. Repeated exposure, especially when the advocate is empathically engaged and professionally responsible for the outcome, can alter the person's internal assumptions about danger, trust, control, and fairness.
In practice, this means the legal professional doesn't just feel sad after hearing traumatic material. The material begins to shape how that professional understands the world. Routine ambiguity may feel threatening. Neutral interactions may be filtered through distrust. Ordinary boundary decisions may start to feel morally loaded.
Why empathy is both necessary and risky
Immigration advocacy depends on empathy. Without it, the interview stays superficial, the declaration remains thin, and the evaluator or attorney may miss the meaning of coercion, captivity, rape, family separation, or chronic persecution.
But empathy also creates the pathway for internalization. The advocate listens closely, imagines the sequence, notices affect, and helps organize the narrative. That is clinically and legally useful. It also increases psychological exposure.
A technically important feature of vicarious trauma is that it often includes cognitive and worldview shifts, not just emotional distress. Guidance from the British Medical Association on signs and coping strategies for vicarious trauma describes increased distrust, heightened vulnerability, helplessness, self-doubt, difficulty maintaining professional boundaries, and preoccupation with clients outside work.
What makes it cumulative
Vicarious trauma usually builds over time. It often doesn't announce itself dramatically. A lawyer may function well through months of high-intensity work and only later notice persistent vigilance, emotional flattening, or a shortened fuse at home.
That cumulative quality is why quick fixes often fail. A weekend off may help fatigue, but it won't necessarily reverse a pattern of intrusive imagery, altered assumptions, and boundary erosion.
The most useful question isn't “Am I stressed?” It's “Has trauma exposure changed how I think, relate, and work?”
For legal teams, that distinction is operational. When symptoms reflect trauma internalization, the response has to include trauma-informed support, not just better time management.
Recognizing the Key Symptom Clusters
Some professionals recognize vicarious trauma symptoms immediately. Most don't. They notice irritability, exhaustion, cynicism, or overinvolvement and assume it's just the job. The problem with that interpretation is that it misses pattern and severity.
Population data suggest this is not a niche issue. One report notes that between 40% and 85% of helping professionals may develop vicarious trauma or high rates of traumatic symptoms, and another study found 34% prevalence among social workers specializing in child protection, as summarized in this field report on vicarious trauma statistics. Legal advocates who spend their days with persecution histories, abuse narratives, and forensic detail should assume exposure risk is real.
A quick visual can help teams spot the pattern early.
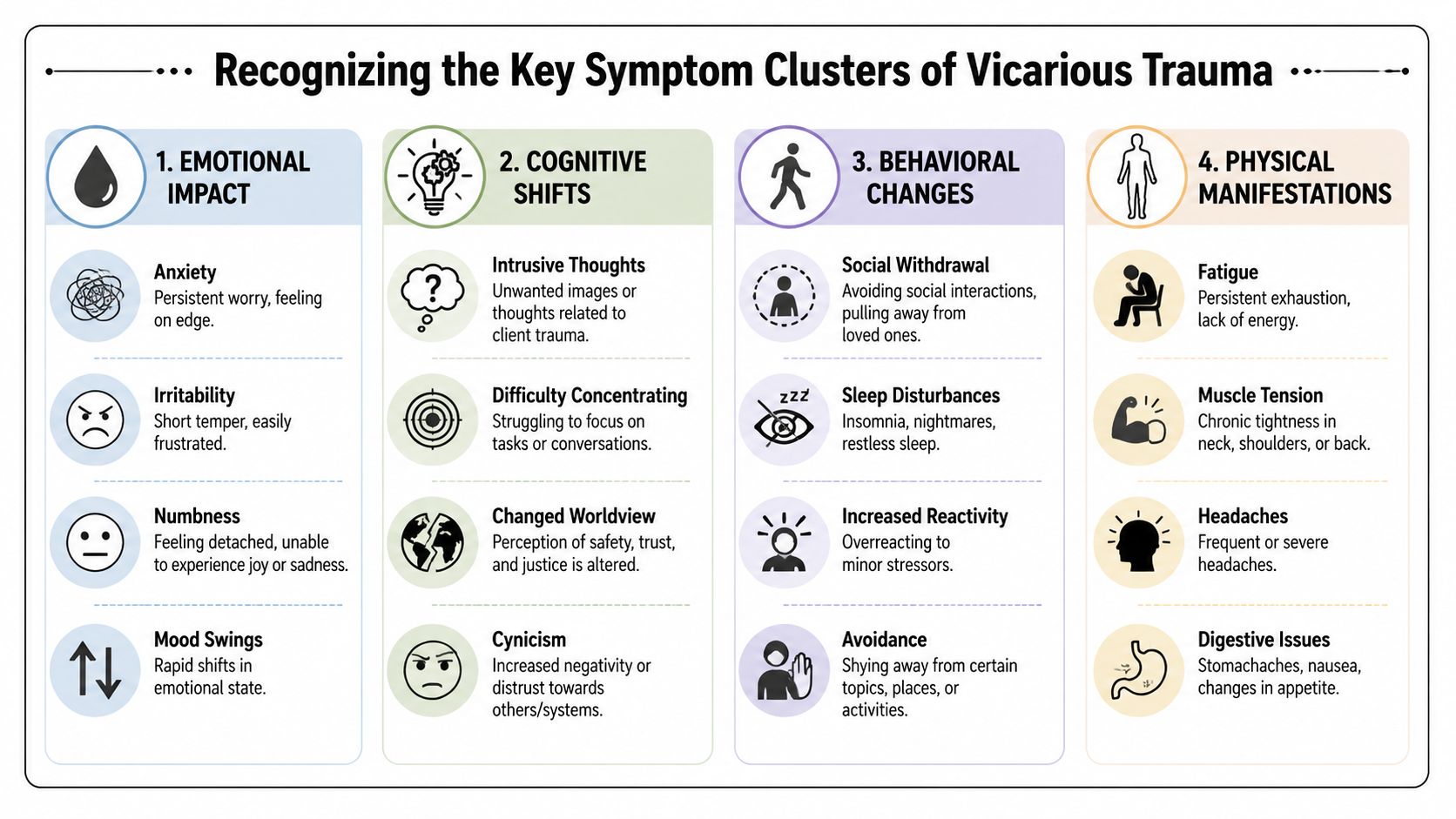
Emotional and cognitive signs
The emotional cluster often includes numbness, fatigue, irritability, and a sense of being on edge. In legal practice, this may look like a lawyer who feels little during a devastating declaration, then snaps at a paralegal over a minor filing issue. The emotional response is not absent. It's displaced, constricted, or poorly regulated.
The cognitive cluster is often more diagnostically useful. Watch for intrusive thoughts, distrust, self-doubt, preoccupation with client safety, and changes in worldview. An attorney may read a routine government notice and react as if it signals catastrophe. A case manager may become unable to stop replaying a client's account while trying to focus on unrelated work.
For some professionals, these trauma-linked patterns overlap with broader autonomic strain. If your team is trying to understand how chronic activation can affect concentration, sleep, and emotional regulation, this overview of nervous system dysregulation is a useful companion concept.
Behavioral and relational signs
Behavioral symptoms usually emerge in work habits and off-duty routines. A skilled advocate may begin delaying affidavit review because trauma-heavy material feels aversive. Another may compulsively overwork, not because the caseload objectively requires it, but because stepping away produces guilt or anxiety.
Common examples in legal settings include:
- Avoidance of client material: A draft sits untouched because reading it will reactivate distress.
- Overchecking and hypervigilance: You repeatedly review facts that were already verified.
- Withdrawal after work: You stop returning calls, decline social contact, and want silence.
- Destructive coping: Sleep problems, emotional shutdown, or other maladaptive habits start to appear.
The Office for Victims of Crime identifies reactions such as emotional numbness, fatigue, sleep problems, irritability, intrusive thoughts, relationship problems, and increased risk of destructive coping behaviors. That symptom profile is reflected in many legal professionals long before they use the term vicarious trauma.
Here is a short educational video that may help staff recognize these patterns in themselves and colleagues.
Physical clues lawyers often dismiss
Physical symptoms are easy to mislabel as ordinary stress. Headaches after affidavit drafting, persistent neck tension after client interviews, restless sleep before testimony prep, or a chronically upset stomach during trauma-heavy weeks can all accompany psychological overload.
When the body starts reacting before the mind has caught up, clinicians take that seriously. Law firms should too.
The key is pattern recognition. A single bad week proves little. Recurring clusters tied to trauma exposure deserve intervention.
Is It Trauma Burnout or Secondary Stress
Mislabeling the problem leads to the wrong fix. If a trauma reaction gets treated as a scheduling problem, the professional may get a lighter week and still feel altered. If simple burnout gets treated as deep trauma injury, the team may miss a solvable workload problem.
The Office for Victims of Crime overview of vicarious trauma is useful here because it frames vicarious trauma as an occupational challenge arising from continuous exposure to trauma, while noting that secondary traumatic stress can overlap with the full PTSD symptom range. That overlap is exactly why legal professionals get confused.
A working differential for legal practice
| Characteristic | Vicarious Trauma (VT) | Burnout | Secondary Traumatic Stress (STS) |
|---|---|---|---|
| Primary driver | Repeated empathic exposure to others' trauma | Chronic workload strain, low control, administrative pressure | Indirect exposure to another person's trauma with trauma-like stress response |
| Core pattern | Internal changes in beliefs, trust, safety, boundaries, and meaning | Emotional exhaustion, reduced efficacy, detachment from work | Symptoms that can resemble PTSD-style reactivity |
| Typical presentation in a law firm | Cynicism about human motives, overidentification with clients, intrusive material outside work | “I can't keep up,” dread of email, depletion, frustration with systems | Acute distress after hearings, interviews, declarations, or graphic records |
| What often helps | Trauma-informed supervision, boundary repair, debriefing, personal treatment support when needed | Caseload adjustment, workflow redesign, staffing changes, protected recovery time | Trauma-informed support, monitoring, and targeted clinical care if symptoms persist |
| Main risk of mislabeling | Treating a trauma response as ordinary stress | Assuming every depleted employee has trauma injury | Missing the cumulative worldview component that points more toward VT |
The shortest practical distinction
Burnout is usually about too much work, too little support, and too little control. Vicarious trauma is more specifically about the psychological imprint of traumatic exposure. Secondary traumatic stress often presents more like a trauma reaction in the classic sense, with acute symptoms that may resemble PTSD-like clusters.
In real life, professionals can experience more than one at the same time. A supervising attorney may be burnt out from volume and also show vicarious trauma symptoms from years of hearing persecution narratives. That complexity is common.
A few decision points help:
- If workload relief helps quickly, burnout may be primary.
- If the person's worldview, boundaries, or trust have shifted, think vicarious trauma.
- If symptoms feel sudden and trauma-like after exposure to a specific case, secondary traumatic stress may be prominent.
Wrong label, wrong intervention. That's why differential thinking matters in supervision and risk management.
How Symptoms Translate to Evidence in Immigration Cases
For immigration lawyers, understanding vicarious trauma symptoms isn't only about protecting staff. It sharpens how you think about evidence. Trauma-related symptoms in a client or qualifying relative can be clinically organized, documented, and translated into legally relevant language when the case calls for it.
Why symptom detail matters in affidavits and evaluations
A client may say, “I can't sleep,” “I'm always on edge,” or “I keep thinking about what happened.” On their own, those statements are real but legally underdeveloped. They need context, chronology, functional impact, and clinical interpretation.
That's especially important in matters where hardship, abuse dynamics, coercion, or trauma sequelae are central. A well-documented evaluation can connect symptoms to daily impairment, relationship disruption, parenting strain, work dysfunction, fear responses, avoidance, or persistent physiological arousal. That makes the record more coherent and more credible.
In immigration practice, symptom descriptions should answer practical questions:
- What does the person experience?
- How often does it occur?
- What triggers it?
- How does it affect work, caregiving, sleep, concentration, or safety?
- How does it relate to the underlying trauma history or separation risk?
What legal teams often miss
Lawyers sometimes collect traumatic facts but miss functional consequences. USCIS and immigration courts don't just need a painful story. They need a documented explanation of what the trauma has done and why that matters in the specific legal framework.
That requires disciplined observation. For example, emotional numbing may affect parenting and marital functioning. Hypervigilance may shape a person's ability to leave home, travel, or engage authority figures. Intrusive thoughts may impair concentration and work consistency. Relationship withdrawal can help explain household instability and dependency patterns.
A careful forensic evaluation goes beyond repeating the client's narrative. It tests consistency, documents symptoms, considers alternative explanations, and translates psychological findings into language that supports the adjudicative question. For attorneys, that means the best mental health evidence is not generic sympathy evidence. It is targeted, structured, and legally responsive.
Sustainable Advocacy and Professional Self-Care
Generic self-care advice usually fails trauma-exposed legal professionals because it treats the problem as vague stress. What helps is more concrete. The goal is to reduce cumulative exposure, strengthen boundaries, and create routines that let the nervous system and the mind exit the case when work ends.
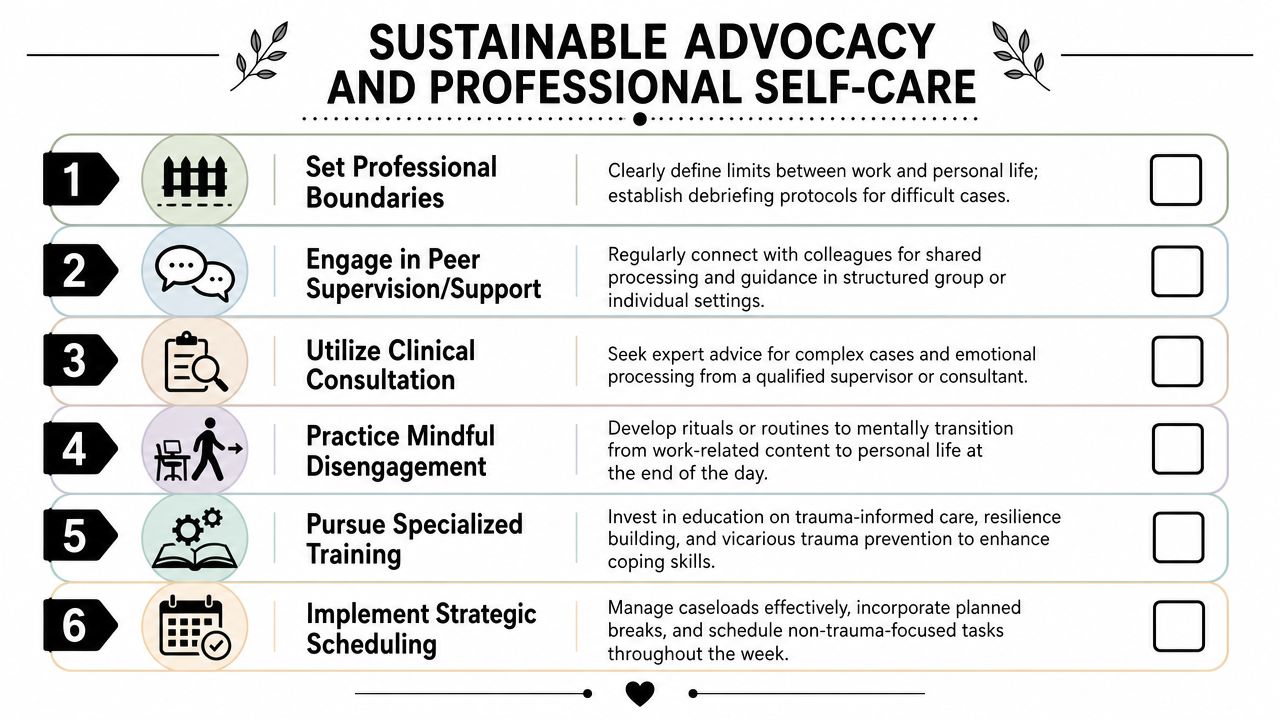
Individual practices that actually fit legal work
Start with the workday itself. Waiting until you're already depleted is too late.
- Use a closing ritual: After a trauma-heavy interview, write the next action step, close the file, and take two minutes to name what is and isn't yours to carry home.
- Segment exposure intentionally: Don't stack multiple graphic client interviews back to back if you can avoid it. Pair trauma-intensive tasks with procedural or administrative work.
- Limit after-hours re-entry: If you must work late, avoid ending the day on the most disturbing material.
- Watch for identity drift: If your entire internal life is becoming organized around clients' danger, your boundaries need repair.
For firms serving diverse communities, broader cultural responsiveness also matters. This discussion of BIPOC Mental Health Month is relevant because workforce sustainability improves when organizations take culturally informed mental health seriously.
Peer and supervisory responses
The strongest buffer is often not solitary coping. It is structured professional support.
A useful debrief is not a casual “rough case” comment in the hallway. It is a short, contained conversation that asks: What was clinically or emotionally difficult here? What are you carrying forward from this interview? What support or redistribution is needed before the next task?
Supervisors should listen for three categories of concern:
- Intrusion signs such as replaying testimony or poor sleep.
- Boundary problems such as overavailability or rescuing impulses.
- Meaning changes such as cynicism, helplessness, or distrust.
A healthy team doesn't wait for collapse. It builds routine places to notice impact before judgment degrades.
Organizational measures firms should normalize
Individual resilience cannot compensate for bad system design. Firms that handle high-trauma matters need protective structure.
Consider these operational safeguards:
- Caseload diversity: Mix trauma-heavy matters with work that is less emotionally saturated.
- Protected consultation time: Complex and disturbing cases shouldn't be processed in isolation.
- Training on trauma exposure: Staff should know what vicarious trauma symptoms look like before they develop them.
- Clear escalation channels: Team members need a path for saying, “This case is affecting me,” without stigma.
What doesn't work is moralizing endurance. Telling professionals to toughen up, be grateful, or “leave work at work” ignores how trauma exposure operates.
Building a Trauma-Informed Practice
A trauma-informed legal practice does more than serve traumatized clients well. It also protects the professionals who must listen, analyze, document, and advocate under repeated exposure to traumatic material.
The central shift is conceptual. Vicarious trauma symptoms are not a side issue. They affect interviewing quality, affidavit development, client trust, supervision, staff retention, and the accuracy of legal judgment. When firms understand the difference between trauma exposure, burnout, and secondary stress, they can choose interventions that fit the actual problem.
The same knowledge improves case strategy. Lawyers who recognize symptom patterns ask better questions, document functional impairment more carefully, and know when a forensic mental health evaluation is necessary to turn distress into legally usable evidence. That strengthens advocacy without sacrificing clinical integrity.
Teams that last in this field build habits around boundaries, debriefing, consultation, and organizational design. They don't treat self-preservation as indulgence. They treat it as competence.
For firms that want to formalize that approach, a practical next step is to review what trauma-responsive interviewing, documentation, and support systems should look like in daily operations. This overview of a trauma-informed care assessment offers a useful framework for that work.
If your firm needs immigration-focused psychological evaluations that document trauma symptoms with clinical precision and legal relevance, Pro Psychological Analysis provides evidence-based assessments for asylum, VAWA, T visa, U visa, and extreme hardship cases. The practice works with attorneys to produce clear, timely, HIPAA-compliant reports that translate complex psychological findings into persuasive immigration evidence.