You may be sitting at home days or weeks after the crash, telling yourself you should be fine by now. The car has been repaired or declared a total loss. The bruises are fading. Friends ask whether you're “okay,” and you say yes, but you notice that you grip the passenger seat at red lights, wake up tense, avoid the route where the collision happened, or feel strangely detached from normal life.
That reaction is more common than many people realize. People can feel traumatized from a car accident even when they weren't hospitalized, didn't lose consciousness, or initially thought the crash “wasn't that bad.” Psychological injury often shows up later, and it often interferes with work, parenting, driving, concentration, and sleep before the person has language for what's happening.
For lawyers, cases get missed or underdeveloped. For clients, people start doubting themselves. The clinical task is to separate normal post-crash distress from a trauma response that deserves treatment and careful documentation. The legal task is to translate those symptoms into evidence that shows causation, functional impairment, and prognosis.
Table of Contents
- The Invisible Injuries After a Car Accident
- Understanding Post-Accident Psychological Trauma
- The Typical Timeline of Symptoms After a Crash
- Recognizing Less Obvious Trauma Responses
- Evidence-Based Treatments and Coping Strategies
- When and How to Seek a Professional Evaluation
- Documenting Trauma for Legal and Immigration Cases
The Invisible Injuries After a Car Accident
A common post-crash story looks like this. Someone walks away from the scene, answers the police officer's questions, calls insurance, and even returns to work. Then, two weeks later, they can't settle down at night. They replay the impact in their head. They start taking side streets to avoid left turns. Their family notices they're more irritable, less patient, and mentally elsewhere.
That doesn't mean they're weak, dramatic, or “making it into something bigger.” It means the nervous system may still be reacting to threat, even after the immediate danger has passed. If you've felt shaken, foggy, keyed up, numb, or unlike yourself, that experience is real. A useful primer on this body-based response appears in this discussion of nervous system dysregulation.
The invisible part matters clinically and legally because trauma after a collision rarely stays confined to emotion. It affects memory, sleep, attention, driving behavior, patience with children, tolerance for noise, and confidence in public. Those are functional losses, not just feelings.
Why car crashes can leave lasting effects
Motor vehicle collisions are not minor stressors to the brain or body. One summary of CDC-based estimates reports that about 1.7 million Americans sustain a TBI each year, about 1,365,000 are treated and released from an emergency department annually, and roughly 5.4 million people in the U.S. live with a TBI-related disability. That same source states that car accidents account for about 14% of U.S. TBI cases and are a leading cause of TBI-related deaths among children and young adults, with severe cases carrying an estimated lifetime cost of more than $4 million per survivor (car accident and brain injury statistics).
Those figures help explain why post-crash symptoms can persist long after the wreckage is cleared.
Practical rule: If a person says, “I survived, so I should be over it,” that's not a clinical conclusion. It's a coping statement.
What clients and attorneys often miss
Visible injury gets documented quickly. Invisible injury often doesn't. People usually seek care for a fracture before they seek care for panic, avoidance, or cognitive fog. By the time they mention the emotional effects, the insurer may argue the symptoms came from something else.
That's why early attention matters. Not because every shaken driver has PTSD, but because untreated trauma can harden into a pattern that disrupts daily life and becomes harder to explain later.
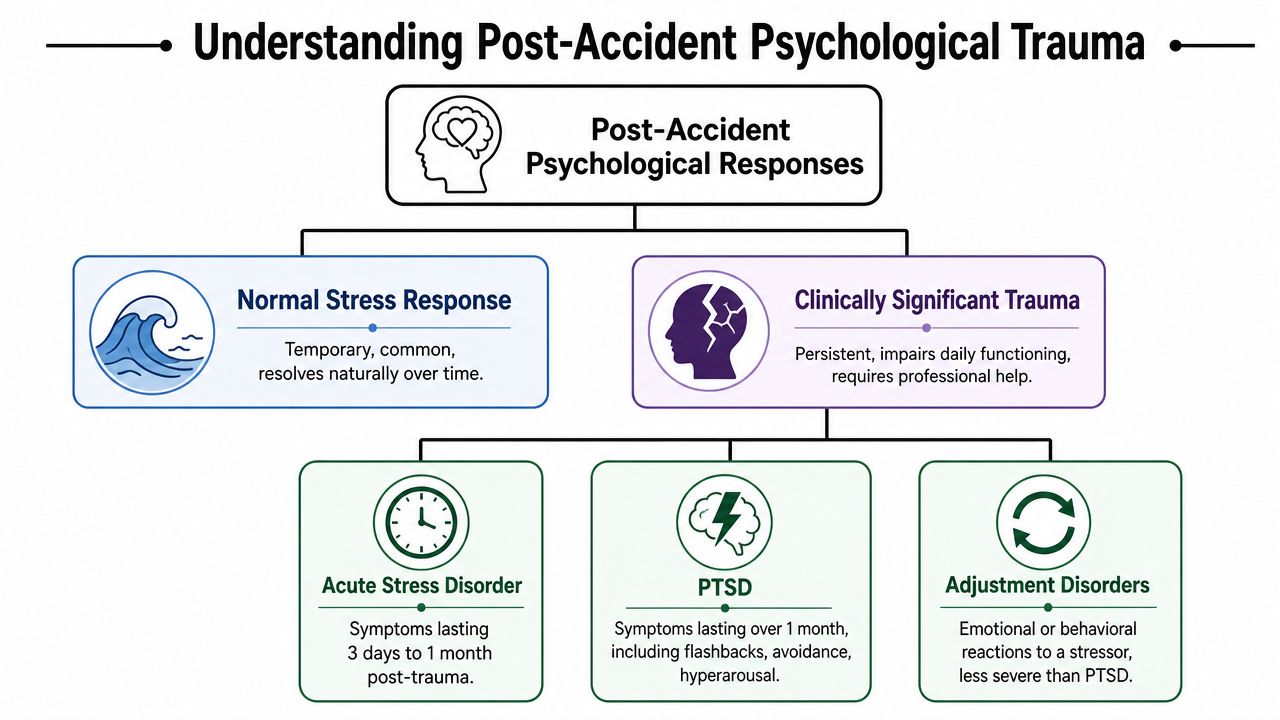
Understanding Post-Accident Psychological Trauma
Right after a crash, many people feel stunned, shaky, tearful, angry, distracted, or unable to stop replaying what happened. That initial response can be normal. A useful analogy is a bruise. A bruise hurts, looks alarming, and then gradually settles. Trauma becomes more clinically significant when the response doesn't settle, or when it starts controlling behavior, mood, and thinking.
A crash can trigger a broad range of post-accident reactions. In the research literature, PTSD rates among motor vehicle crash victims have been reported anywhere from 8% to 46%, and one peer-reviewed study of moderately and severely injured vehicular crash patients found PTSD in 27.5% at 6 months and 24.3% at 12 months. The same body of research notes that road traffic incidents are a common trigger for trauma symptoms, with some summaries reporting about 25% to 33% may develop PTSD within 30 days, while another review states roughly 9% of survivors develop PTSD (peer-reviewed review of PTSD after motor vehicle crashes).
Normal distress versus a disorder
Normal distress usually has these features:
- It's tied to the event: The person feels upset when thinking about the collision.
- It gradually eases: Sleep, appetite, concentration, and driving confidence start to improve.
- It doesn't keep expanding: The person isn't shrinking their life more and more each week.
Clinically significant trauma looks different:
- Symptoms persist or intensify: Instead of fading, they start shaping daily decisions.
- Function drops: Work errors increase, driving stops, relationships become strained.
- Avoidance grows: The person stops taking highways, then local roads, then refuses to ride in a car.
The symptom clusters that matter
When clinicians assess trauma after a crash, they don't just ask, “Are you anxious?” They look for patterns.
| Symptom cluster | What it can look like after a crash |
|---|---|
| Re-experiencing | Flashbacks, nightmares, sudden body panic at screeching brakes |
| Avoidance | Refusing to drive, avoiding the intersection, skipping appointments that require travel |
| Mood and thinking changes | Guilt, fear, detachment, hopelessness, trouble remembering parts of the event |
| Hyperarousal | Startling easily, sleeping poorly, scanning traffic constantly, irritability |
Why labels matter less than impairment
A person may meet criteria for Acute Stress Disorder, PTSD, or another trauma-related condition. Another person may not meet full criteria but still be significantly impaired. That distinction matters in treatment planning, but from a practical standpoint, the first question is simpler: is the crash still interfering with how this person lives?
A diagnosis organizes symptoms. It doesn't create them.
That's why lawyers should pay attention not only to the formal label, but also to commuting problems, concentration lapses, childcare disruptions, missed work, and fear-based changes in routine.
The Typical Timeline of Symptoms After a Crash
The timeline after a collision is rarely linear. Some people feel terrible immediately and then improve. Others seem composed at first and begin struggling later, once the adrenaline wears off and normal routines return.
The first days and weeks
In the immediate aftermath, shock, confusion, anger, sleep disturbance, and intrusive images are all common. The brain is trying to process a sudden threat. Many survivors describe feeling “wired and exhausted at the same time.” That combination is typical early on.
During the first month, clinicians look closely at whether symptoms are receding or becoming organized into a more persistent trauma pattern. Intrusive memories, fear while riding in a car, and jumpiness can all occur in this period without meaning the person will go on to develop chronic PTSD.
The three-month marker
One clinically important benchmark is 3 months. Guidance for motor-vehicle-injury survivors notes that early intrusive symptoms are common in the first weeks and that most acute stress symptoms after a crash resolve within 3 months. At the same time, an estimated 8% to 29% of survivors develop PTSD, and co-occurring depression, mild TBI, and chronic pain can complicate diagnosis because irritability, poor sleep, and concentration problems may overlap with trauma symptoms (Phoenix Australia guidance for motor vehicle accident survivors).
That means “wait and see” has limits. If the person still can't drive comfortably, keeps reliving the crash, or functions poorly well past the early recovery period, the problem deserves a more formal evaluation.
Delayed onset is real
Some survivors don't look obviously distressed at first. They're busy with repairs, medical appointments, work leave, or family logistics. Later, they begin having panic in traffic, difficulty sleeping, or a rising sense of dread whenever they approach the crash location.
This delayed pattern often confuses both clients and counsel. People assume that if symptoms weren't immediate, they must not be related. Clinically, that's too simplistic. Trauma responses can surface after the person has enough distance from the crisis to feel the impact.
What to monitor over time
A simple tracking frame is often more useful than speculation:
- Driving behavior: Are routes shrinking? Is the person avoiding highways, rain, night driving, or intersections?
- Work capacity: Are they making mistakes, calling out, or struggling with meetings and deadlines?
- Home life: Are they more reactive, withdrawn, or unable to rest?
- Body symptoms: Is pain, dizziness, or sleep disruption making the emotional picture harder to interpret?
For legal documentation, a timeline matters. Symptom onset, progression, attempts to cope, and points of deterioration often become central to causation analysis.
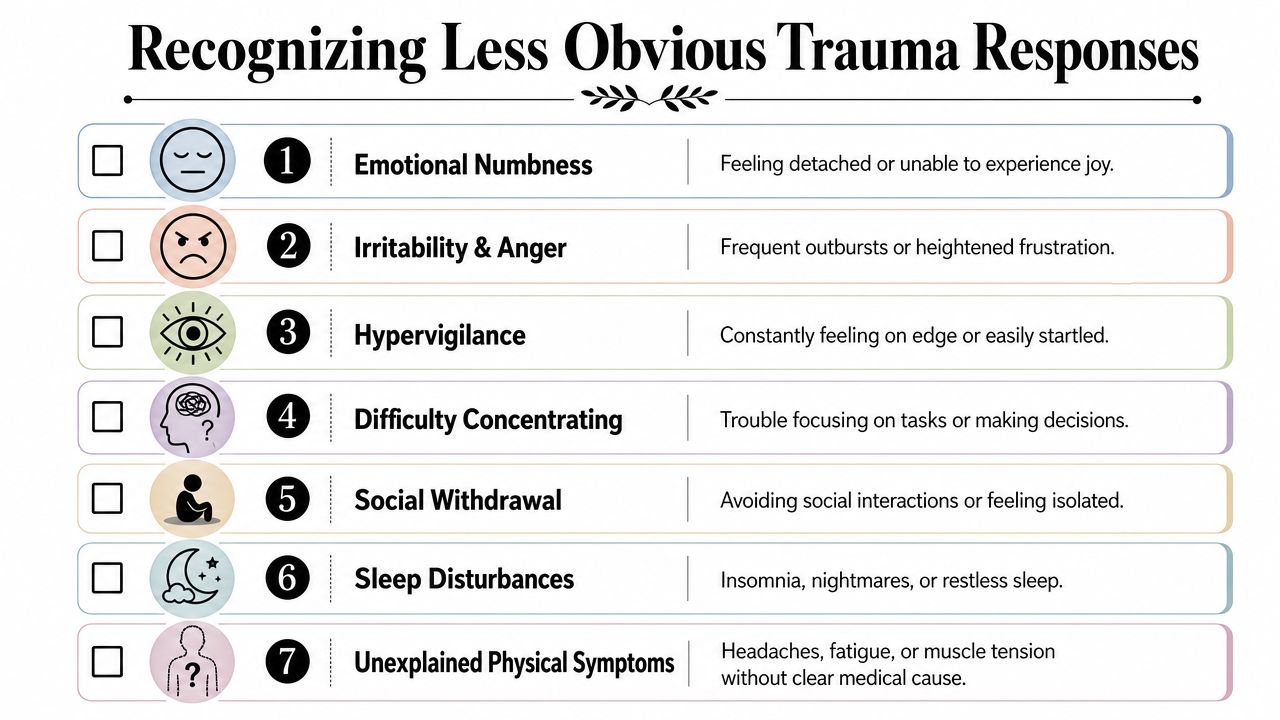
Recognizing Less Obvious Trauma Responses
Many people assume trauma after a wreck has to look dramatic. They expect flashbacks, screaming, or a total refusal to leave the house. In practice, some of the most impairing cases are quieter. The person is still working, still parenting, still showing up. They're just doing all of it with fear, exhaustion, avoidance, or cognitive strain that nobody around them fully sees.
When the crash didn't seem severe
A common misconception is that only catastrophic collisions cause major psychological fallout. That's not how trauma risk works. Risk isn't limited to severe crashes. People with mild traumatic brain injury, prior psychiatric history, or a subjective sense that they might die can be at higher risk, and one summary notes that a concussion can double the likelihood of developing PTSD within a year, even when the person wasn't hospitalized (discussion of overlooked post-accident trauma risk).
The phrase I hear often is, “I know other people have had worse accidents.” Clinically, that comparison doesn't answer the question. The relevant issue is how this person's brain and body processed threat.
Symptoms that don't look like classic PTSD
Less obvious trauma responses often show up as changes in function rather than obvious fear.
- Driving phobia: The person can ride as a passenger but cannot merge, turn left, or pass a truck.
- Cognitive fog: They reread emails, forget appointments, or lose track mid-conversation.
- Irritability: Family members notice a short fuse that wasn't there before.
- Emotional numbing: The person says they feel flat, detached, or “not like myself.”
- Sleep disruption: Not always nightmares. Sometimes it's trouble falling asleep because the body won't settle.
Some crash survivors don't say “I'm traumatized.” They say, “I can't focus,” “I dread driving,” or “I'm exhausted all the time.”
The overlap problem
Mild TBI, chronic pain, depression, and trauma can mimic one another in daily life. A person with concussion symptoms may report headaches, reduced concentration, sleep trouble, and irritability. A person with trauma may report the same things. Many have both.
That overlap creates two risks. One is undertreatment, where everyone assumes the symptoms will pass. The other is sloppy overlabeling, where every symptom gets called PTSD without considering concussion, medication effects, pain, grief, or prior mental health history.
A practical triage question
If you aren't sure whether someone is traumatized from a car accident, ask this: Has the crash changed how they function, even if they don't look outwardly distressed?
If the answer is yes, it deserves clinical attention. The problem may be PTSD, a driving phobia, an adjustment problem, post-concussive symptoms, depression, or a mixture. What matters is that the impairment is real and identifiable.
Evidence-Based Treatments and Coping Strategies
Treatment works best when it matches the actual problem. A person with panic while driving needs a different plan than someone with nightmares, guilt, and emotional numbness. A person with concussion-related fog may need a slower pace and more coordination between providers. Good care isn't generic reassurance. It's targeted, structured, and practical.

What tends to help
For clinically significant trauma, trauma-focused psychotherapy is usually the center of treatment. In plain terms, that means therapy that helps the brain process the crash memory instead of repeatedly reacting as if the danger is still present.
Common approaches include:
- Trauma-focused CBT: Helps the person identify threat-based beliefs, reduce avoidance, and build a more accurate sense of safety.
- EMDR: Uses structured recall and bilateral stimulation to help process traumatic material. Many clients find it less overwhelming than retelling the story repeatedly. A plain-language overview of the benefits of EMDR is useful for people considering that option.
- Exposure-based work for driving fear: Gradual return to driving in planned steps, rather than forced immersion or total avoidance.
What usually doesn't help is passive avoidance. Taking longer routes, refusing to drive, or waiting indefinitely for confidence to “come back on its own” often makes the fear more entrenched.
A grounded approach to coping day to day
Immediate coping tools aren't a replacement for therapy, but they can lower distress enough for the person to function.
| Situation | Skill | Why it helps |
|---|---|---|
| Panic in traffic | Name five things you can see, four you can feel, three you can hear | Brings attention back to the present |
| Body tension before driving | Slow exhale longer than inhale | Signals the body to downshift |
| Intrusive replay of the crash | Say the date, location, and that the event is over | Reorients the brain to current safety |
| Avoidance of driving | Break the task into steps | Builds mastery without flooding |
Graded exposure works better than all-or-nothing
A smart return-to-driving plan is gradual. For example:
- Sit in the parked car.
- Ride with a trusted driver on a quiet street.
- Drive around the block.
- Take a familiar route in daylight.
- Reintroduce more difficult conditions, one variable at a time.
That progression isn't glamorous, but it works better than pushing too hard and reinforcing panic.
A brief guided resource may help some readers get started:
Clinical caution: If driving fear is paired with dizziness, headaches, concentration problems, or suspected concussion, don't assume it's “just anxiety.” Coordinate care.
What recovery often requires
Recovery usually involves repetition, not a breakthrough moment. The person practices tolerating reminders without fleeing them. They rebuild confidence through action. They learn to distinguish present risk from remembered danger.
That's also why legal teams should be careful with simplistic narratives. “She's going to therapy” doesn't capture the work. Better documentation describes what she still avoids, what she can now do that she couldn't do before, and what remains impaired.
When and How to Seek a Professional Evaluation
Many people wait too long because they think they need to be in constant crisis before seeing a psychologist. They don't. An evaluation is appropriate when symptoms are persistent, confusing, functionally disruptive, or legally relevant.
Red flags that justify evaluation
Consider a formal assessment when any of these are present:
- Symptoms aren't fading: Fear, intrusive memories, irritability, or sleep problems continue rather than ease.
- Daily function is impaired: The person avoids driving, misses work, struggles to parent, or withdraws socially.
- The picture is mixed: Trauma symptoms overlap with concussion, chronic pain, or depression.
- The case needs documentation: Counsel needs a diagnosis, causation opinion, impairment analysis, or prognosis.
Seeking an evaluation isn't an admission that the person is permanently damaged. It's a way to clarify what's happening.
What a clinician actually does
A good trauma evaluation does more than collect complaints. The psychologist asks about the collision, the person's subjective experience of threat, symptom onset, medical course, prior mental health history, current functioning, and what changed after the crash. The goal is differential diagnosis, not just sympathy.
For PTSD after a crash, clinicians commonly use the 17-item PTSD Checklist, often with cutoff scores of 44 or 50 to flag likely PTSD for follow-up, and a structured interview such as the CAPS is described as a gold-standard assessment because it rates symptom frequency and intensity across the PTSD symptom set (clinical discussion of PCL cutoffs and CAPS).
What attorneys should look for
For legal purposes, not every mental health note carries the same weight. A strong evaluator should be able to address:
- Causation: Why the symptoms are linked to the crash rather than vaguely attributed stress.
- Diagnosis: Whether the person meets criteria for PTSD or another condition.
- Functional impairment: How symptoms affect work, driving, relationships, sleep, and concentration.
- Method: What records were reviewed, what interview methods were used, and how conclusions were reached.
A useful report doesn't just say someone is anxious. It explains how the anxiety shows up, why it matters, and why the evaluator reached that conclusion.
Timing matters
Early evaluation can improve treatment access and preserve a cleaner record. Later evaluation can still be valuable, especially in delayed-onset cases, but earlier is usually easier to explain and document.
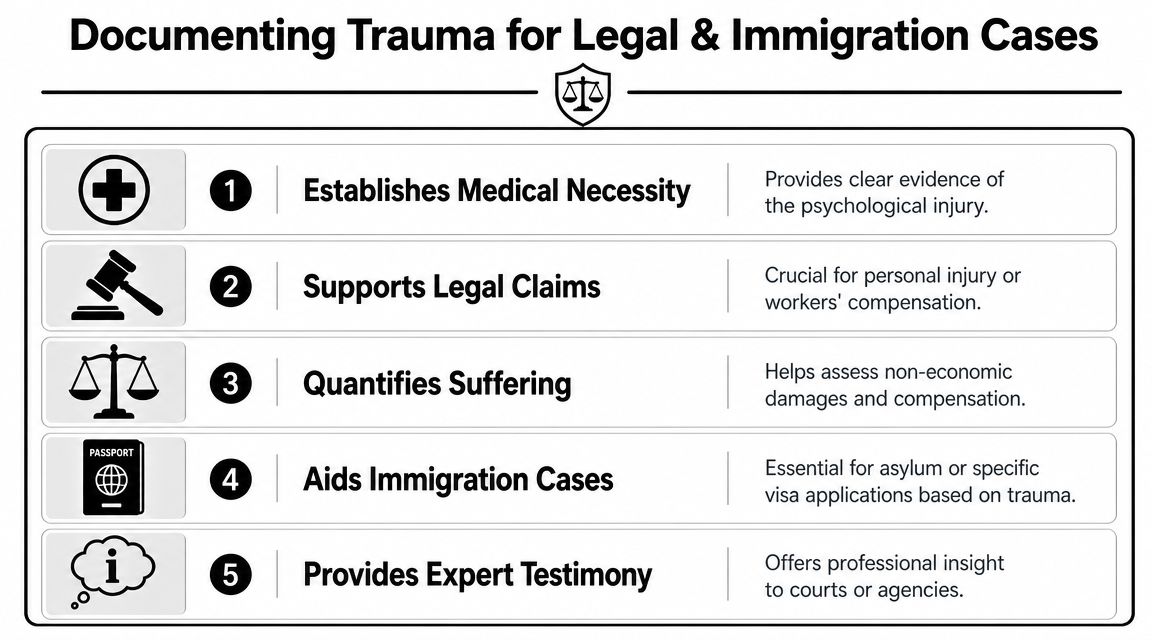
Documenting Trauma for Legal and Immigration Cases
Psychological trauma only helps a legal case when it is translated into organized, credible evidence. That applies in personal injury matters, and it also matters in immigration cases where a car accident may intersect with a history of abuse, victimization, or vulnerability. A person may present after a collision with worsening fear, sleep disruption, avoidance, and concentration problems that affect testimony, memory consistency, and daily functioning.
What makes documentation persuasive
A casual therapy note can be helpful, but it usually isn't enough on its own. Legal decision-makers often need something more structured. A forensic-style psychological evaluation can connect the dots between event, symptoms, diagnosis, and real-world impairment in a way ordinary treatment records often do not.
Useful documentation typically addresses:
- Temporal relationship: When symptoms began and how they changed over time
- Functional impact: Effects on work, parenting, commuting, sleep, and social functioning
- Diagnostic clarity: Whether symptoms fit PTSD, acute stress, depression, concussion-related complications, or a combination
- Consistency: Whether the person's account matches records, observed behavior, and collateral information
For attorneys, detailed medical documentation strengthens argument because it shows not only that the client suffered, but how that suffering is clinically understood and why it matters.
For survivors and counsel
Survivors should describe concrete examples, not just labels. “I avoid the highway where I was hit” is stronger than “I have anxiety.” “I forgot client calls and stopped driving my children to school” is stronger than “I'm stressed.”
For lawyers, the key request is specificity. Ask the evaluator to address diagnosis, causation, functional impairment, treatment recommendations, and prognosis in language that is clinically sound and legally usable. In immigration matters, that same precision can help explain trauma-related functioning in asylum, U visa, T visa, VAWA, or hardship-related contexts when the accident is part of the psychological picture.
If you need a formal psychological evaluation that translates trauma into clear, court-ready analysis, Pro Psychological Analysis provides evidence-based assessments for immigration and other legal matters. Their reports are designed to document clinical symptoms, trauma history, functional impairment, and diagnostic conclusions in a format attorneys can use effectively.