You probably have a client like this on your desk right now. They plainly struggle. The family tells you they can't retain new information, can't follow even simple test prep, or shut down when asked basic questions. Yet the records are thin, the treating doctor wrote a vague note, and the legal file still doesn't answer the one question USCIS cares about most: why this person cannot meet the English and civics requirements because of a qualifying impairment.
That gap is where many otherwise legitimate cases weaken.
As a forensic psychologist, I've seen the same pattern repeatedly. The problem usually isn't that the applicant lacks a real condition. The problem is that the medical documentation reads like ordinary clinical paperwork, while USCIS reviews Form N-648 as a legal record. A diagnosis, by itself, rarely carries the case. Functional explanation does.
Good medical certification for disability exceptions isn't just about completing a form. It's about translating clinical facts into a defensible theory of impairment, one that fits the legal standard and anticipates skepticism. If the documentation doesn't connect symptoms, duration, testing limitations, and learning barriers in a clear chain, the case is easier to doubt than to approve.
Table of Contents
- Why Medical Certifications Are More Than Just Paperwork
- Defining the Medical Certification for Disability Exceptions
- Choosing the Right Clinician for USCIS Certification
- Building the Clinical Evidence for an N-648 Waiver
- Navigating Accommodations vs True Disability Exceptions
- Avoiding Common Pitfalls in Your N-648 Submission
- Strengthening Your Case with Specialized Psychological Evaluations
Why Medical Certifications Are More Than Just Paperwork
An attorney calls after a naturalization interview goes badly. The client has a long history of confusion, poor memory, and limited ability to learn new material. A primary care provider filled out the N-648, but the explanation was short, diagnosis-heavy, and nonfunctional. The form listed conditions. It didn't show how those conditions prevented the applicant from learning or demonstrating English and civics.
That's the practical problem. USCIS doesn't need proof that a person is unwell in the abstract. USCIS needs a persuasive record that ties the impairment to the testing barrier.
In practice, Form N-648 works less like a routine clinic form and more like evidentiary writing. Attorneys who treat it that way usually build cleaner cases. Clinicians who understand that distinction tend to produce stronger certifications. If you want a useful primer on what counts as supporting records generally, this overview of medical documentation in legal and clinical settings is a helpful companion.
What weak submissions usually miss
The weakest certifications often share the same flaws:
- They name a diagnosis without describing function. “Depression,” “dementia,” or “developmental disability” alone doesn't answer whether the person can learn, retain, or express the required knowledge.
- They rely on broad conclusions. Statements like “patient is unable to take the test” don't explain how the clinician reached that opinion.
- They sound therapeutic, not forensic. Clinical notes often aim to support treatment. N-648 writing has to support adjudication.
Practical rule: If the form would make sense to a treating team but not to an immigration officer, it's probably underdeveloped.
Why this matters strategically
A strong N-648 gives the legal file structure. It can explain inconsistent school history, failed test preparation, communication problems, memory deficits, disorientation, or severe psychiatric interference in a way that aligns with the statute and USCIS review standards. It can also prevent the attorney from leaning too heavily on sympathetic facts that don't legally carry the waiver.
That's why I advise attorneys to stop thinking of the certification as an attachment and start treating it as a central theory-of-the-case document. When the clinical record is precise, the legal argument becomes easier to defend. When the clinical record is vague, the attorney ends up trying to rescue a medical opinion that was never built for scrutiny.
Defining the Medical Certification for Disability Exceptions
Form N-648 is not a general hardship note, and it isn't a substitute for weak test preparation. It is the federal government's formal mechanism for documenting a disability-based exception to the naturalization English and civics requirements. USCIS states that the condition must be medically determinable and must have lasted or be expected to last at least 12 months, and the form is meant to show why the applicant cannot meet those requirements because of a physical or developmental disability or mental impairment, not because of illiteracy, age, or education level alone, as outlined in Project Citizenship's Form N-648 packet for medical professionals.
What the form is
Think of the N-648 as a functional incapacity certification. Its job is to establish that a qualifying condition exists and that the condition meaningfully blocks the applicant from learning or demonstrating the required material.
That's an important distinction. The form is not asking whether the applicant has had a difficult life, limited schooling, or a language barrier. Those facts may be relevant context, but they are not the legal basis for the disability exception.
What the form is not
A useful analogy is this. A doctor's excuse from work says someone is sick. An N-648 has to do much more. It has to explain why the condition causes a specific legal consequence: inability to satisfy the naturalization testing requirements.
That difference matters in older applicants especially. Age can coexist with genuine neurocognitive impairment, but age by itself is not the impairment. Illiteracy can coexist with trauma, intellectual limitations, or developmental disability, but illiteracy alone is not the basis for the exception.
The strongest certifications separate nonqualifying background factors from the qualifying medical impairment, then show how the impairment drives the limitation.
The threshold question attorneys should ask early
Before referring for certification, ask one hard question: Is the barrier medical and function-based, or is it primarily educational, linguistic, or social?
That question protects the case. If the answer is mostly educational deprivation, the N-648 route may be the wrong route. If the answer is medical, the evaluation needs to show duration, diagnostic basis, and real-world effect on learning, recall, comprehension, or communication.
A quick screening table can help:
| Issue | Usually enough for N-648 by itself | Needs deeper medical analysis |
|---|---|---|
| Limited formal education | No | Yes |
| Advanced age alone | No | Yes |
| Medically determinable mental impairment | Potentially | Yes |
| Developmental disability | Potentially | Yes |
| Physical condition affecting communication or testing ability | Potentially | Yes |
The legal standard is narrower than many families assume. That's not a defect in the process. It's the point of the process.
Choosing the Right Clinician for USCIS Certification
Not every well-meaning provider is the right certifier. Under USCIS rules, Form N-648 may be certified only by a licensed medical doctor, doctor of osteopathy, or clinical psychologist in the United States or its territories. The condition must be medically determinable, must have lasted or be expected to last at least 12 months, and the form must explain the causal nexus between symptoms and the inability to learn English and or civics rather than relying on diagnosis alone, as described in the OMB supporting materials for Form N-648.
Eligibility is only the first filter
The fact that a clinician is permitted to sign the form doesn't mean that clinician is the strongest choice. At this juncture, legal strategy and clinical fit should line up.
A primary care physician may know the patient well and have longitudinal records. That can help. But if the central issue is trauma, cognition, psychosis, intellectual limitations, or complicated symptom presentation, a clinician with deeper assessment training may produce a more defensible explanation.
If you want a broader framework for matching referral questions to evaluator skill, this discussion of clinical assessment and how it supports decision-making is useful.
Match the evaluator to the impairment
Different clinicians bring different strengths.
- Clinical psychologists are often especially useful when the case turns on cognition, memory, trauma symptoms, intellectual functioning, or the distinction between poor education and true impairment.
- MDs or DOs may be stronger when the record centers on neurological disease, major medical illness, physical disability, medication effects, or complex multisystem conditions.
- A treating specialist can be valuable when that specialist can explain the condition in concrete functional terms rather than merely confirm treatment history.
What attorneys should look for before referral
Don't ask only, “Can this provider sign?” Ask these instead:
- Can the provider explain function clearly? USCIS needs plain-language connection, not jargon.
- Can the provider tolerate scrutiny? A good certifier can justify conclusions if the case is questioned.
- Does the provider know the difference between diagnosis and nexus? That difference often decides whether the form persuades.
A strategically chosen clinician doesn't just verify illness. The clinician helps the record make sense.
I often advise attorneys to think in terms of evidentiary fit. If the client's presentation is subtle, mixed, or easy to underestimate, the wrong provider can unintentionally flatten the case. The right provider can identify the actual mechanism of impairment and document it in language that aligns with adjudication.
Building the Clinical Evidence for an N-648 Waiver
A diagnosis starts the analysis. It doesn't finish it.
The center of a persuasive N-648 is the causal nexus. In plain terms, that means the clinician must explain how the applicant's symptoms produce the specific inability to learn, retain, or demonstrate English and civics knowledge. Without that bridge, the form reads like a list of health problems followed by a legal conclusion.
What a robust assessment actually does
A careful evaluation usually pulls from more than one source. The clinician may rely on interview data, behavioral observations, record review, mental status findings, and, when appropriate, formal psychological or cognitive testing. The exact mix depends on the condition and on what question the case needs answered.
What matters is not volume. What matters is whether the assessment identifies the mechanism of failure.
For example, these are very different pathways:
| Clinical issue | Functional legal relevance |
|---|---|
| Severe memory impairment | The person cannot retain civics content over time |
| Impaired attention and concentration | The person cannot sustain learning or respond consistently during testing |
| Receptive language deficits | The person cannot understand questions well enough to demonstrate knowledge |
| Disorganized thinking or severe psychiatric symptoms | The person cannot reliably process, retrieve, and express information |
Why the revised form changed the writing burden
USCIS revised the N-648 process in a policy update that expanded the form from 12 to 23 questions, removed some prior prompts about daily-life functions, dates of diagnosis, severity descriptions, and a pre-existing relationship with the patient, and allowed the clinician to indicate the need for an oath waiver on the same form, eliminating separate medical documentation for that purpose, according to Immigration Policy Tracking's summary of the N-648 revision.
That change matters because a longer form does not automatically mean a clearer one. In practice, it increases the need for disciplined reasoning. The clinician has more places to be precise, and more opportunities to be inconsistent.
What works and what doesn't
Here's the contrast I watch for in reports and draft forms.
Weak approach
- Lists diagnoses
- Uses broad phrases like “difficulty learning”
- Assumes severity is obvious
- Offers conclusions without examples
Strong approach
- Describes observed or documented deficits
- Explains how those deficits affect learning, recall, expression, or comprehension
- Distinguishes long-term impairment from temporary distress
- States whether the limitation applies despite support, repetition, or ordinary instruction
If the clinician cannot explain the pathway from symptoms to test incapacity in plain English, the case is not ready.
Clinical details that tend to strengthen the nexus
Not every case needs every element, but these features usually help:
Symptom specificity
“Memory problems” is too broad. What kind of memory problem? Encoding, delayed recall, retrieval, working memory?Task-specific explanation
Can the applicant understand spoken questions? Retain basic facts? Shift attention? Tolerate the demands of testing?Consistency across sources
The history, observations, and records should point in the same direction.Differential reasoning
The clinician should separate true impairment from low literacy, language exposure, or anxiety that doesn't rise to disabling incapacity.
Here, forensic habits matter. The goal is not to produce the longest report. The goal is to produce an explanation that survives legal reading.
Navigating Accommodations vs True Disability Exceptions
This is one of the most misunderstood parts of the N-648 analysis. Some applicants have a genuine impairment and still do not qualify for a disability exception because reasonable accommodations would allow them to take and pass the test.
USCIS materials state that applicants who can meet the English and civics requirements with reasonable accommodations do not need Form N-648, and examples include sign language interpreters, extended time, and off-site testing. That distinction leaves a strategic gap for many cases because the key issue is not just whether a disability exists, but whether accommodations can bridge the learning or testing barrier. In practice, this makes the N-648 more of a functional-capacity document than a diagnosis form, as explained in the Hartford Public Library guidance on Form N-648.
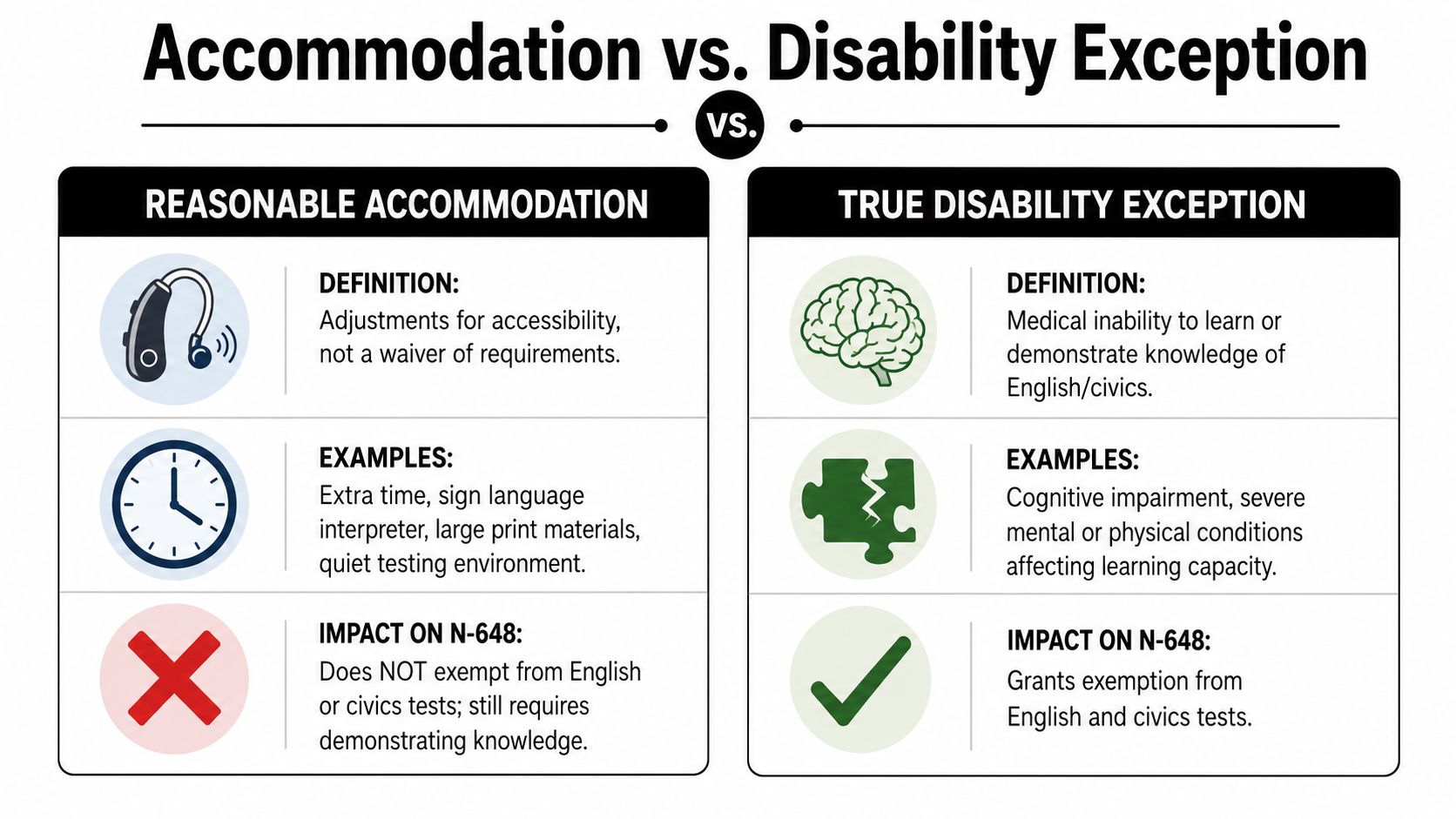
The practical difference
An accommodation modifies how the applicant takes the test. A disability exception removes the need to satisfy the English and civics requirements because the applicant cannot meet them even with support.
That's a major legal distinction.
Side-by-side comparison
| Question | Accommodation case | Disability exception case |
|---|---|---|
| Can the applicant learn the material with support? | Often yes | No, not in a meaningful or reliable way |
| Is the problem access to the test format? | Often yes | No, the problem is deeper than format |
| Would extra time, interpretation support, or environment changes solve it? | Possibly | No |
| What must the clinician prove? | Need for support | Inability despite accommodation |
Examples attorneys can use to frame referral decisions
Likely accommodation case
A deaf applicant may need a sign language interpreter. That need alone does not establish inability to learn civics or English.Potential exception case
An applicant with major neurocognitive decline may be unable to retain even repeatedly taught information. Extra time won't fix failure to encode or retrieve material.Borderline case
An applicant with trauma symptoms may struggle during testing, but if the evidence suggests they can still learn and demonstrate knowledge with modifications, the N-648 theory becomes weaker.
When I review these cases, the decisive question is usually simple: does support make testing possible, or does the impairment make learning itself unattainable?
Why this distinction changes legal strategy
If the attorney pursues an exception where an accommodation is more appropriate, the filing can look overstated. If the attorney ignores the accommodation issue entirely, the medical form may fail to answer an obvious USCIS concern.
Clinicians should address that head-on. They should explain not only what the applicant cannot do, but also why accommodations would not overcome the relevant deficits. That reasoning is especially important in cognitive and psychiatric cases where the person may appear superficially intact in conversation but still be unable to handle sustained learning, recall, or organized responding under test conditions.
Avoiding Common Pitfalls in Your N-648 Submission
Most N-648 problems are predictable. They don't usually come from dramatic fraud indicators. They come from ordinary sloppiness, vague reasoning, or a mismatch between clinical language and legal needs.
The fastest way to strengthen a submission is to review it like opposing counsel would.
Before and after mistakes that matter
Before: Diagnosis only
“Applicant has depression and anxiety.”
After: Functional explanation
Describe how symptoms interfere with concentration, memory, language processing, or the ability to demonstrate knowledge.Before: Conclusions without support
“Patient cannot take the exam.”
After: Clinical reasoning
State what data support that conclusion. Interview findings, records, observations, and testing should point to the same limitation.Before: Soft, hedged language
“May have difficulty” or “appears limited.”
After: Defensible language
If the evidence supports it, state the limitation clearly and specifically.
A pre-submission review lens
Ask these questions before filing:
- Does the form identify a qualifying impairment rather than a social or educational disadvantage?
- Does it explain duration clearly?
- Does it show causation, not just coexistence?
- Does it address why ordinary accommodations aren't enough, if that issue is relevant?
- Does the wording stay consistent throughout the form?
Pitfalls I see in practice
Some are subtle.
| Pitfall | Why it hurts the case | Better approach |
|---|---|---|
| Boilerplate language | Sounds generic and unexamined | Use applicant-specific facts |
| Overreliance on sympathy | Doesn't meet the legal standard | Focus on impairment mechanics |
| Confusing poor education with disability | Invites denial | Separate background limits from medical incapacity |
| Incomplete narrative | Leaves USCIS to fill gaps | Make the reasoning explicit |
Review standard: Every major conclusion in the form should answer “how do you know?” without forcing the adjudicator to guess.
One more caution. Don't let the clinician write as if the audience is another clinician. USCIS officers need direct statements, not dense shorthand. Clear language is not simplistic language. In this setting, clear language is disciplined evidence.
Strengthening Your Case with Specialized Psychological Evaluations
Some N-648 matters are straightforward. Many are not. The hard cases usually involve mixed presentations: trauma plus cognitive decline, developmental limits masked by social adaptation, psychiatric symptoms that fluctuate, or medical records that confirm illness but don't explain testing incapacity.
That's where specialized psychological work becomes valuable. A forensic-style evaluation is built to answer legal questions, not just treatment questions. It can examine memory, attention, comprehension, executive functioning, trauma-related interference, and response style in a way that helps the legal file hold together.

A good specialized evaluation also helps attorneys avoid two common extremes. One is under-documenting a legitimate disability. The other is overstating a case that really belongs in the accommodations lane. The evaluation should narrow that uncertainty and translate clinical findings into language that an adjudicator can use.
For cognitive, trauma-related, and neuropsychological questions, a comprehensive neuropsychological evaluation can be especially helpful when the central issue is whether the applicant can learn, retain, or express required knowledge in any reliable way.
Confidentiality matters too. These evaluations often involve sensitive psychiatric, medical, and trauma histories. The work should be HIPAA-compliant, tightly documented, and focused on the legal issue at hand rather than padded with irrelevant clinical detail.
The strongest N-648 cases usually share one trait. The clinical evidence doesn't merely say the applicant is impaired. It shows, step by step, why the impairment prevents compliance with the naturalization testing requirements.
When your case depends on proving that link with precision, Pro Psychological Analysis provides specialized, evidence-based immigration evaluations designed for legal scrutiny. The practice partners with attorneys to produce clear, HIPAA-compliant reports that translate trauma, cognitive impairment, and psychiatric symptoms into persuasive clinical findings for USCIS and immigration court.