You're often in this position when a trauma case gets harder, not easier, the more documents you collect. The client has a long history of abuse, coercion, trafficking, detention, or family violence. Their affidavit is credible but fragmented. Dates drift. Disclosure comes in pieces. Opposing counsel or an adjudicator may read that inconsistency as weakness when, clinically, it can be part of the trauma picture itself.
That's where a complex PTSD assessment becomes more than a diagnosis exercise. In immigration practice, the evaluation has to do two jobs at once. It must be clinically rigorous enough to withstand scrutiny, and it must translate that rigor into findings that help USCIS or the immigration court understand hardship, harm, credibility context, and functional impact.
A weak trauma letter rarely fails because the client lacked suffering. It fails because the method is thin, the differential diagnosis is vague, the impairment analysis is underdeveloped, or the report never links symptoms to the legal question. A strong C-PTSD evaluation does the opposite. It organizes chronic trauma into a defensible clinical formulation and then turns that formulation into legally useful evidence.
Table of Contents
- What Is Complex PTSD and Why It Matters in Court
- Anatomy of a Forensically Sound C-PTSD Assessment
- Distinguishing C-PTSD from Similar Diagnoses
- How a C-PTSD Diagnosis Strengthens Immigration Claims
- What to Expect from a Court-Ready C-PTSD Report
- Managing Ethical and Logistical Complexities
- A Strategic Checklist for Your Next Trauma Case
What Is Complex PTSD and Why It Matters in Court
Complex PTSD is not just “more PTSD.” In current diagnostic practice, it has a distinct framework. A key milestone is that CPTSD is recognized in the ICD-11 but not in the DSM-5, and ICD-11 separates it from PTSD by requiring PTSD symptoms plus disturbances in self-organization, involving affect regulation, self-concept, and relationships, as described by the U.S. Department of Veterans Affairs overview of complex PTSD.
For legal work, that distinction matters because many immigration clients don't present as people who suffered one isolated traumatic event and then developed fear-based symptoms. They often present as people whose identities, relationships, emotional regulation, and day-to-day functioning were shaped by chronic coercion or repeated victimization. If you need a concise clinical background on that broader trauma pattern, this overview of complex trauma is a useful companion.
Why the diagnosis matters legally
In court, labels matter less than fit. A diagnosis has persuasive force when it explains facts the record already contains but doesn't yet organize well. C-PTSD often does that better than standard PTSD when the client's presentation includes chronic shame, unstable attachment, emotional flooding, numbing, dissociation, or a pattern of returning to dangerous relationships.
A useful analogy is this. PTSD can look like a deep wound from a specific injury. C-PTSD often looks like the body and mind adapting to repeated injury over time. That distinction helps an adjudicator understand why the client may appear guarded, contradictory in minor details, intensely self-blaming, or unable to describe harm in a neat chronological sequence.
Practical rule: If the client's impairment extends beyond fear and re-experiencing into identity, attachment, and emotional regulation, a C-PTSD framework may describe the case more accurately than PTSD alone.
What the court can understand from a C-PTSD formulation
A well-formed C-PTSD opinion helps the trier of fact understand three things at once:
- Why disclosure is fragmented. Chronic trauma survivors often disclose gradually, especially when abuse involved dependency, threats, or humiliation.
- Why behavior can appear counterintuitive. Returning to an abuser, delaying reporting, minimizing harm, or appearing emotionally flat can be trauma-consistent rather than credibility-damaging.
- Why the injury is pervasive. The condition affects more than symptom distress. It often affects trust, self-worth, parenting, employment stability, and the ability to handle legal processes.
That makes the diagnosis strategically important in asylum, VAWA, U visa, T visa, and hardship contexts. The legal system doesn't need a more dramatic narrative. It needs a more precise one.
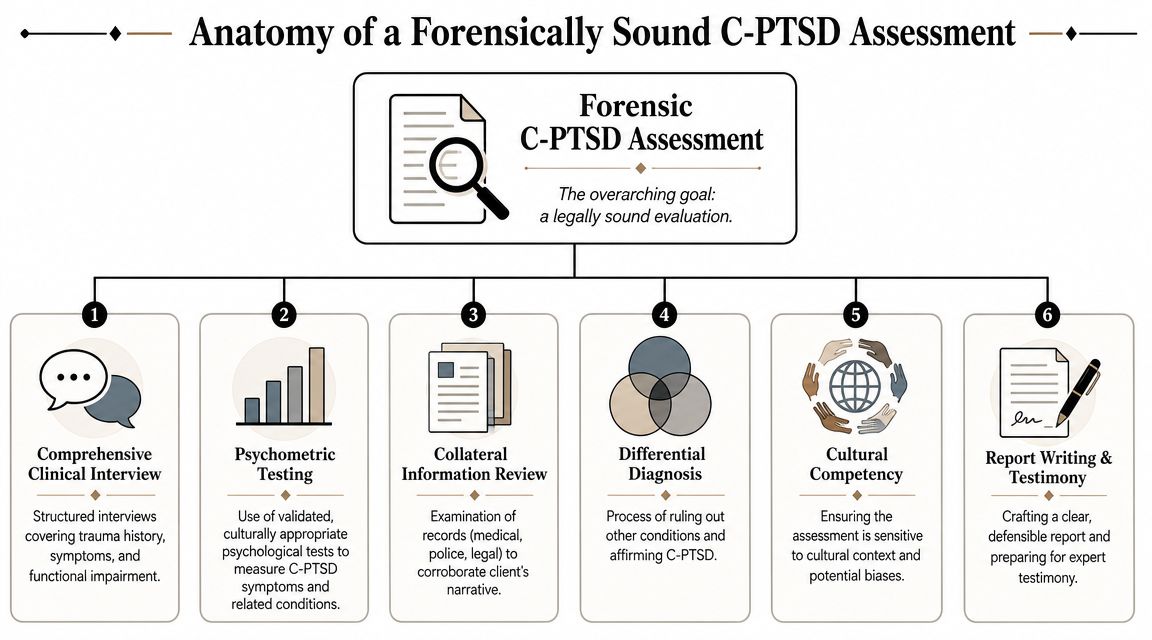
Anatomy of a Forensically Sound C-PTSD Assessment
A court-facing trauma evaluation should never read like a treatment note expanded into letterhead. It needs a method. The strongest complex PTSD assessment uses multiple data sources and makes clear why each source was used.
The core building blocks
The first building block is the clinical interview. In forensic settings, that interview has to be structured enough to cover trauma exposure, symptom development, functional impairment, migration history, and alternate explanations, while still being flexible enough to avoid pushing the client into a rehearsed or collapsed account. Attorneys who want a quick refresher on that method usually benefit from this explanation of a structured interview.
The second building block is psychometric testing. For ICD-11 C-PTSD, the key screening framework is the International Trauma Questionnaire, or ITQ. It is a widely used 18-item self-report tool that includes 6 PTSD items and 6 disturbance-of-self-organization items, with impairment questions, and a provisional CPTSD result requires PTSD criteria plus endorsement across the DSO domains and functional impairment, as summarized by the VA guidance on complex PTSD assessment.
Later in the process, it can also help to understand how prior screening fits into the picture. One recent study reported that a PCL-5 score of 51 or higher may serve as an initial indicator of possible ICD-11 CPTSD, but only as a screening threshold, not a diagnosis, and the result should be followed by an ITQ or trained clinical interview, according to the Hendrikx paper on PCL-5 cutoff for CPTSD.pdf).
A well-run assessment also reviews collateral records. Medical notes, police reports, affidavits, shelter records, school records, detention records, and prior declarations can't substitute for an interview, but they do serve another essential forensic function. They test consistency across time and context.
What strengthens admissibility
The report becomes more persuasive when the evaluator builds a trauma timeline. That timeline doesn't just list events. It tracks onset, escalation, symptom emergence, avoidance patterns, disruptions in work or caregiving, and the client's changing ability to function or seek help.
What doesn't work is a vague summary that says the client “reports trauma consistent with PTSD” and stops there. For court purposes, the evaluator should be able to explain:
- What symptoms are present
- How those symptoms meet the chosen diagnostic framework
- Why competing diagnoses were considered
- How the symptoms impair functioning
- How the findings relate to the legal issue
The most persuasive report is usually the one that shows its work.
That's the difference between a document that merely sounds compassionate and one that can survive careful review.
Distinguishing C-PTSD from Similar Diagnoses
Differential diagnosis is where trauma evaluations often become either credible or vulnerable. In immigration cases, that matters because the wrong label can distort the client's narrative. It can also give the government an opening to argue that the evaluator relied on a broad trauma story instead of disciplined clinical reasoning.
Authoritative guidance notes substantial overlap between C-PTSD, PTSD, and borderline personality disorder, and stresses that assessment must pay attention to affect dysregulation, shame-based self-concept, relational disturbance, dissociation, and functional impairment rather than trauma exposure alone. It also notes that some clients disclose in avoidant or masked ways that can understate impairment on a brief screen, as discussed in this clinical review of C-PTSD assessment overlap.
Where overlap creates risk
The most common mistake is assuming that severe trauma history automatically answers the diagnosis question. It doesn't. Diagnosis turns on symptom pattern, organization, duration, and impairment.
The second mistake is treating emotional volatility or unstable relationships as proof of borderline personality disorder without asking whether those patterns are better understood as trauma-linked adaptations. In forensic work, the evaluator has to show why one formulation explains the available evidence better than another.
A good differential diagnosis doesn't erase overlap. It explains it.
Differential diagnosis C-PTSD vs PTSD vs BPD
| Feature | Complex PTSD (C-PTSD) | PTSD | Borderline Personality Disorder (BPD) |
|---|---|---|---|
| Core framework | PTSD symptoms plus disturbances in self-organization | Trauma-related fear-based syndrome | Personality organization marked by pervasive instability |
| Trauma connection | Commonly understood in relation to prolonged or repeated trauma | Often tied to traumatic exposure without the added DSO pattern | Trauma may be present, but diagnosis is not defined by trauma framework alone |
| Emotional regulation | Chronic dysregulation that often reflects survival adaptation | Distress may spike around reminders, avoidance, and hyperarousal | Dysregulation may be broader, more pervasive, and not fully organized around trauma response |
| Self-concept | Persistent shame, guilt, worthlessness, or damaged identity | Negative beliefs may occur, but not necessarily the enduring identity disturbance seen in C-PTSD | Identity disturbance may be prominent, but requires separate personality-level analysis |
| Relationships | Persistent distrust, detachment, dependency, or difficulty sustaining safe bonds | Avoidance and withdrawal may occur, often around reminders or threat | Instability in relationships may be intense and reactive across settings |
| Forensic question | Are the broader identity and relational symptoms best explained by chronic trauma? | Are classic PTSD criteria met without the full DSO picture? | Are the longstanding interpersonal and affective patterns better explained by personality structure than trauma adaptation? |
In practice, the strongest evaluator doesn't force certainty where the data are mixed. If the record is incomplete, the report should say so, explain the limits, and still give a reasoned opinion. That restraint often makes the opinion more persuasive, not less.
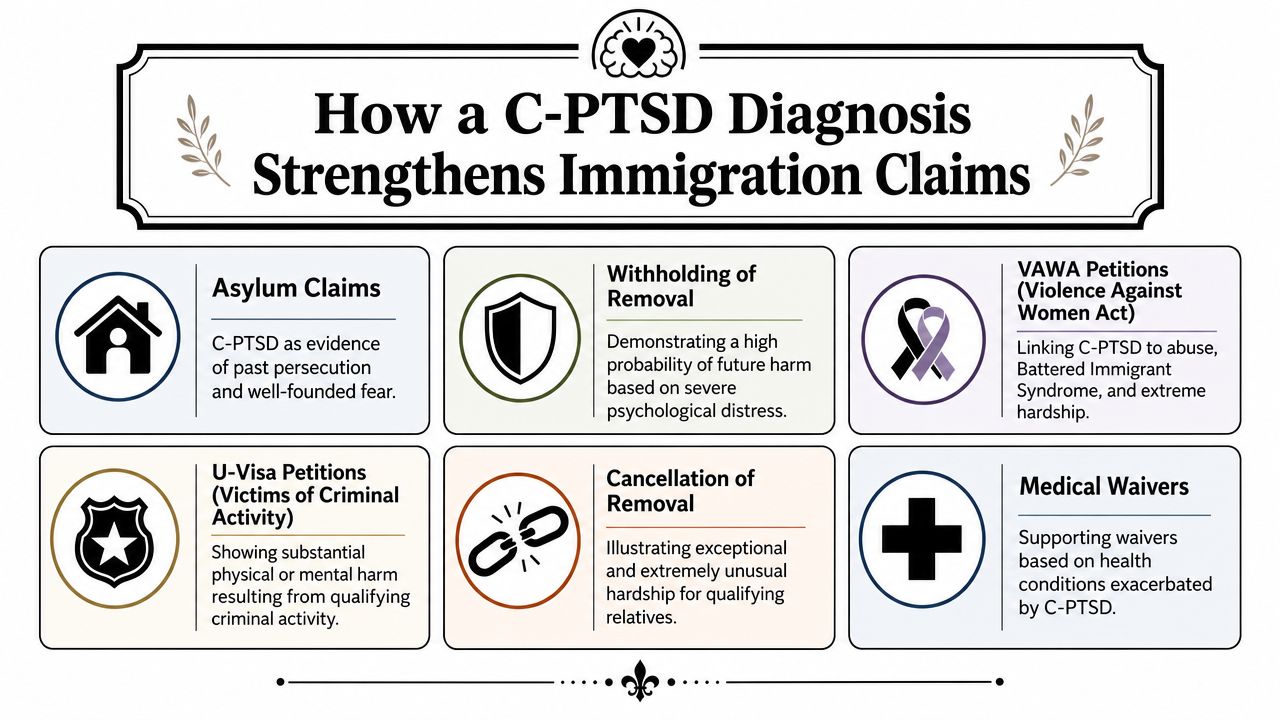
How a C-PTSD Diagnosis Strengthens Immigration Claims
A C-PTSD diagnosis helps an immigration case when it does more than name suffering. Its real value lies in showing how the psychological injury operates and why that injury matters under the legal standard at issue.
Why impairment drives legal value
Many reports fall short. They describe symptoms but never convert those symptoms into findings about work, parenting, concentration, trust, help-seeking, or daily functioning. That leaves the legal team with language that sounds serious but doesn't do enough evidentiary work.
A stronger framework focuses on impairment. The ITQ itself requires functional impairment, and clinical guidance emphasizes that the key legal issue is often not only whether C-PTSD is present, but how the evaluator can convert fluctuating symptoms into defensible findings about the client's ability to work, maintain relationships, and function in daily life, as discussed in this overview of screening for complex PTSD and documenting impairment.
How symptoms map onto common forms of relief
For asylum, a C-PTSD formulation can help explain the subjective experience of fear, ongoing arousal, avoidance, and damaged self-concept after persecution or abuse. It can also contextualize why testimony may be emotionally constrained or chronologically disorganized without implying fabrication.
For VAWA cases, the DSO domains are often especially useful. Relational disturbance can illuminate coercive control, trauma bonding, and the lingering effects of extreme cruelty. Shame-based self-concept may explain why the client stayed, recanted, or minimized abuse.
For U visa and T visa cases, the report can document substantial mental harm tied to qualifying victimization. A careful evaluator will usually connect symptoms to concrete life consequences, such as inability to trust authorities, episodes of emotional flooding during official interviews, or difficulty maintaining basic daily stability.
For hardship-based matters, the most persuasive findings usually involve practical limitations rather than diagnosis labels. Adjudicators need to understand what happens if this person is separated from support, returned to a threatening environment, or expected to function without treatment continuity and safety.
- The strongest linkage is behavioral. Show what the client can and cannot do reliably.
- The second strongest linkage is temporal. Show when symptoms emerged and how they track the harm.
- The weakest linkage is abstract severity language. “Severe trauma” alone doesn't answer a legal question.
When the report explains impairment in concrete terms, the legal argument becomes easier to draft and easier to defend.
What to Expect from a Court-Ready C-PTSD Report
A court-ready report should read like a disciplined expert product, not a sympathetic summary. The report needs to make its forensic role obvious from the opening pages.
The sections that should be there
A strong report usually includes a clear forensic purpose statement, the referral question, limits of confidentiality, dates of contact, and the sources of information reviewed. That source list matters. It tells the adjudicator whether the opinion rests only on a single conversation or on a broader evidentiary foundation.
The clinical narrative should then cover the trauma history, symptom development, current presentation, relevant psychosocial history, and mental status observations. In a C-PTSD case, the evaluator should also address the symptom pattern that supports the formulation, especially where the injury extends into emotional regulation, self-concept, and relationships.
A useful report also includes a direct diagnostic reasoning section. That section should explain why the evaluator selected C-PTSD, why other reasonable alternatives were considered, and what limits apply if information remains incomplete. Judges and officers may not use clinical language daily, but they understand transparent reasoning.
What weak reports tend to miss
The most common omission is the nexus analysis. That's the part where the evaluator links the clinical findings to the legal issue. If the legal question concerns persecution, extreme cruelty, substantial mental harm, or hardship, the report should say how the symptoms and impairment bear on that issue.
Another frequent weakness is overreliance on conclusions without methodology. If the report says the client has C-PTSD, the reader should be able to see the basis for that opinion in the interview data, test results, observed functioning, and collateral review.
Here's a simple quality check attorneys can use:
- Method stated clearly. The report identifies interview procedures, testing, and records reviewed.
- Diagnostic logic visible. The evaluator explains how the criteria are met and why alternatives don't fit as well.
- Impairment described concretely. The report addresses work, relationships, daily functioning, and legal-process functioning.
- Legal relevance explicit. The evaluator doesn't leave the court to guess why the findings matter.
When those pieces are present, the report doesn't just sound professional. It becomes easier to rely on in briefing, declarations, and testimony.
Managing Ethical and Logistical Complexities
Some of the hardest trauma evaluations fail for reasons that aren't clinical. The problem is often logistical or ethical. The client didn't understand the forensic role. The attorney sent too little background. The virtual setting wasn't private. The referral question was never narrowed.
Why ethics and structure matter in high-risk referrals
Structured, ethical assessment matters because trauma exposure is common while the disorder itself is not automatic. Reported probable CPTSD prevalence has ranged from 0.5% in a German general-population one-month estimate to 39.5% among women survivors of intimate partner violence, and a Danish psychiatric outpatient sample reported 36%, according to the European Society for Traumatic Stress Studies fact sheet on CPTSD prevalence. In referral populations common to immigration practice, that means clinicians shouldn't assume C-PTSD, but they also shouldn't miss it through a rushed screen. For attorneys working through those issues, a trauma-informed framework like this discussion of trauma-informed care assessment can improve referrals.
That principle affects consent and preparation. Clients need to understand that a forensic evaluation is not treatment, that the information is being gathered for a legal purpose, and that the evaluator may ask clarifying questions that feel detailed or repetitive because accuracy matters.
Attorney practices that improve the evaluation
The best referral packets usually include the retainer or referral question, client declaration drafts, prior affidavits, relevant filings, police or medical records, and a short memo identifying the legal theory. That gives the evaluator context without dictating conclusions.
For virtual evaluations, a few practices matter a great deal:
- Confirm privacy first. The client should be in a confidential space, not near family members, employers, or the alleged abuser.
- Verify identity and location. That protects the integrity of the evaluation and helps if safety concerns arise.
- Plan for interpretation carefully. The interpreter must understand the forensic setting and translate faithfully rather than summarize.
- Prepare without coaching. Explain the process, tell the client to answer truthfully, and avoid scripting symptom descriptions.
The attorney's job is to prepare the client for the setting, not the content.
Ethically, that distinction is essential. Good preparation reduces fear and confusion. Coaching distorts the data and weakens the case. When attorneys and evaluators stay disciplined on that line, the final opinion is stronger and more defensible.
A Strategic Checklist for Your Next Trauma Case
When a client presents with prolonged abuse, coercive control, trafficking, family violence, detention trauma, or repeated victimization, the clinical question shouldn't be limited to “Do they have PTSD?” The sharper question is whether the pattern suggests a condition that also affects identity, regulation, and relationships, and whether that pattern can be documented in a way the court can use.
Use this checklist early, not after the declaration is finished.
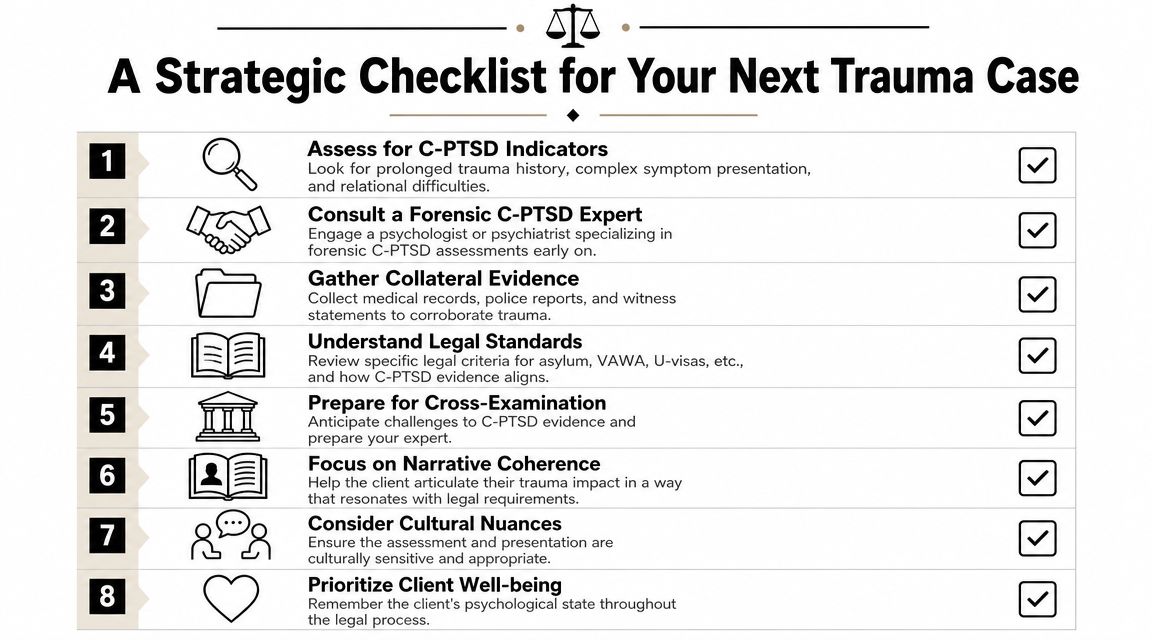
- Screen for the right presentation. Look for chronic trauma history, shame, attachment disruption, emotional dysregulation, and fragmented disclosure.
- Choose a forensic evaluator, not just any therapist. The report must show method, differential diagnosis, and legal relevance.
- Send a real referral packet. Include declarations, filings, records, and the exact legal question you need answered.
- Expect impairment analysis. A useful report explains effects on work, caregiving, relationships, concentration, and daily functioning.
- Read for nexus. The report should connect symptoms and functional limits to the legal standard, not leave that translation entirely to briefing.
- Prepare the client ethically. Explain purpose, confidentiality limits, and process. Don't script answers.
- Anticipate scrutiny. The cleaner the method, the easier it is to defend inconsistencies, explain trauma-linked behavior, and support credibility context.
A strong complex PTSD assessment gives the adjudicator something rare in trauma litigation. It provides a coherent explanation for why the client presents the way they do, grounded in a diagnostic framework and tied to observable impairment. That's often what turns a painful story into persuasive evidence.
Immigration cases involving chronic trauma need more than a sympathetic letter. They need a forensically sound evaluation that can stand up in USCIS filings and immigration court. Pro Psychological Analysis partners with attorneys to deliver evidence-based psychological assessments for asylum, VAWA, U visa, T visa, and hardship cases, with careful attention to clinical rigor, confidentiality, and the legal questions that decide outcomes.