You may be looking at a file right now where the physical injury is obvious, but the client's presentation is making the case harder. They miss appointments. Their declaration is thin. They say they “don't remember” important periods, or they answer in a flat, detached way that can read as evasive, reflecting exhaustion and emotional shutdown. In immigration practice, that pattern shows up often when the injury is part of the underlying harm.
Attorneys usually know how to document fractures, scars, emergency treatment, or surgical records. The harder issue is the psychiatric aftermath that develops after the injury and then starts interfering with testimony, daily functioning, and case preparation. Post injury depression can change how a client works, sleeps, thinks, organizes, relates to family, and participates in legal proceedings. If nobody names it and documents it carefully, the record can look inconsistent when it is clinically coherent.
For U Visa, T Visa, VAWA, and asylum matters, this isn't just a treatment issue. It's an evidentiary issue. A well-prepared report can connect the injury, the depressive syndrome that followed, and the resulting impairment in a way USCIS and the court can understand.
Table of Contents
- The Hidden Factor in Your Client's Injury Case
- Identifying Post-Injury Depression Symptoms and Timeline
- The Assessment Toolkit for Defensible Legal Reports
- Distinguishing Depression from Related Conditions
- Evidence-Based Treatments and Impact on Prognosis
- Documenting Functional Impairment for USCIS
The Hidden Factor in Your Client's Injury Case
A client survives an assault, workplace accident, detention-related injury, domestic violence episode, or trafficking-related harm. The medical records confirm the event. Months later, the attorney expects the client to be more stable because the visible injuries have improved. Instead, the client is more withdrawn, slower to respond, less able to describe what happened, and less consistent in daily functioning.
That pattern often gets misread.
Some attorneys assume the client is uncooperative. Some providers assume the person is discouraged about pain or finances. Family members may say the client is “not the same person.” In clinical practice, those observations can point to a depressive disorder that developed after the injury and is now shaping behavior in ways that directly affect the case.
Why this matters in immigration matters
In immigration reports, the central question usually isn't whether a person feels sad. It's whether the psychological consequences of the injury are real, diagnosable, and functionally significant. A credible report has to answer practical questions:
- Can the client give a coherent history? Depression can reduce concentration, slow recall, and flatten emotional expression.
- Can the client maintain work or caregiving roles? When energy, motivation, and sleep deteriorate, routine functioning often follows.
- Can the client reliably assist counsel? A person may want to participate fully and still fail because initiating tasks feels overwhelming.
- Does the psychiatric condition fit the timing of the injury? The narrative must show more than distress. It must show a clinically plausible course.
Practical rule: If a client's post-injury behavior makes the legal case harder to develop, treat that behavior as potential evidence, not just a case management problem.
The legal value of recognizing post injury depression is that it can unify facts that otherwise seem scattered. Missed work, social withdrawal, poor follow-through, emotional numbness, reduced self-care, and diminished participation in treatment can all become understandable once they're evaluated within a diagnostic framework.
What doesn't work
A short letter saying the client is “depressed due to trauma” rarely carries much weight. It doesn't clarify diagnosis, onset, severity, or impairment. It also doesn't show that the evaluator considered other explanations, such as PTSD, adjustment disorder, or neurocognitive effects from head injury.
What works is disciplined documentation. The report should identify the injury, trace the symptom course, describe daily impairment, and explain why the diagnosis fits better than competing formulations. That's what turns a mental health opinion into persuasive evidence.
Identifying Post-Injury Depression Symptoms and Timeline
A visible injury has a treatment course that attorneys can often map easily. Depression after injury rarely follows that same straightforward pattern. It may begin subtly, intensify after the acute crisis passes, and persist even when the physical healing process appears to be moving in the right direction.
To orient the timeline, this visual is useful:
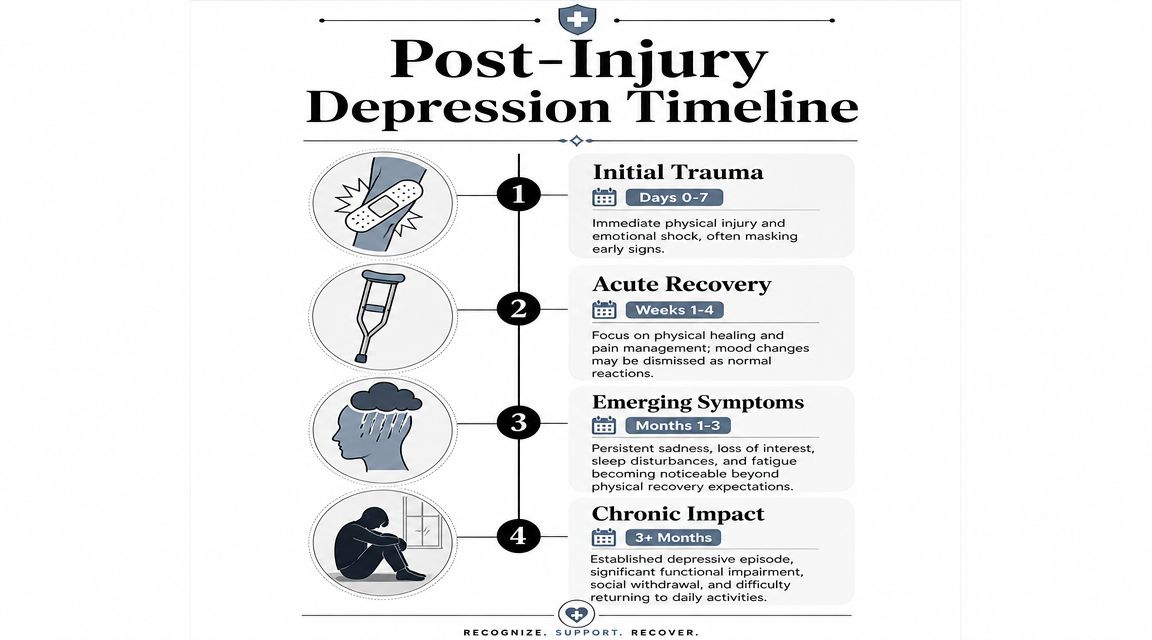
What depression looks like after an injury
Clinically, the core features are familiar, but their presentation in injury cases is easy to miss. Look for persistent low mood, loss of interest or pleasure, reduced motivation, fatigue, hopelessness, guilt, sleep disruption, appetite change, psychomotor slowing, poor concentration, and feelings of worthlessness. Some clients don't volunteer “sadness” at all. They describe themselves as empty, numb, tired, or unable to care about anything.
That distinction matters. Normal frustration after an injury usually tracks with pain, inconvenience, or temporary limitation. Post injury depression is broader. It affects identity, drive, relationships, and the ability to function across settings, not just emotional reaction to discomfort.
A frequent legal problem is mistaking depressive symptoms for attitude. A client who gives one-word answers may be slowed and anhedonic, not oppositional. A parent who stopped participating in family life may not be indifferent. They may be unable to initiate ordinary activity.
Depression after injury often behaves like a psychological echo. The body absorbs the first impact, and the mood disorder becomes fully visible later.
The timing data support that clinical caution. In a prospective cohort study of 559 patients hospitalized for traumatic brain injury, 53.1% met criteria for major depressive disorder at least once during the first year after injury, and point prevalence ranged from 31% at 1 month to 21% at 6 months, showing that depression remains common across the post-injury year (JAMA study on depression after traumatic brain injury).
Later in the section, this overview video may help attorneys explain the concept to staff or clients:
Why timing matters in legal records
The symptom timeline often creates avoidable credibility disputes. A client may look emotionally “better” in the emergency phase because survival, pain control, and logistics dominate attention. Weeks or months later, when medical contact drops and life consequences become real, the depression becomes more obvious.
That means attorneys should compare records across time, not just at intake.
- Early records may understate mood symptoms. Acute care notes usually prioritize physical stabilization.
- Middle-period records often show the shift. Follow-up visits may start mentioning sleep problems, low energy, crying, withdrawal, or inability to resume normal routines.
- Collateral accounts become valuable. Family members often notice reduced engagement before the client can describe it clearly.
When the timeline is built carefully, apparent inconsistencies stop looking suspicious. They begin to look clinically expected.
The Assessment Toolkit for Defensible Legal Reports
A defensible report doesn't rely on a single impression. It uses a small set of tools that answer different questions. One tool measures symptom severity. Another establishes diagnosis. Another helps sort out whether concentration and memory complaints belong to depression, brain injury, trauma response, or some combination.

What a strong evaluation includes
The first layer is usually a standardized depression screener, such as the PHQ-9. In legal settings, the value of a screener isn't that it replaces diagnosis. It doesn't. Its value is that it gives the evaluator a structured snapshot of symptom burden using a recognized instrument. That helps anchor the report in more than general observation.
The second layer is the clinical interview, which is where the report becomes useful to counsel. A structured or semi-structured interview clarifies onset, symptom progression, prior psychiatric history, treatment history, functional decline, and the relationship between the injury and current presentation. Attorneys who want to understand why this part matters can review a concise overview of a structured clinical interview in psychological evaluations.
The third layer is selective cognitive or neurobehavioral screening when the facts suggest head trauma, concussion, or persistent cognitive complaints. This isn't necessary in every case. It is necessary when the record includes memory loss, slowed processing, headaches, confusion, or inconsistent recall that could reflect more than depression.
What weak reports tend to miss
Weak reports often fail in one of three ways.
- They skip chronology. A diagnosis without a symptom timeline invites challenge.
- They don't tie symptoms to function. Saying someone has depression is less persuasive than explaining how that depression interferes with work, parenting, self-care, and legal participation.
- They ignore alternatives. If PTSD, adjustment disorder, chronic pain, or TBI effects aren't considered, the report looks incomplete.
A better report usually addresses the following points directly:
- Injury context: What happened, what medical response followed, and what changed afterward.
- Symptom course: Whether symptoms emerged immediately, gradually, or after a brief period of apparent stability.
- Functional consequences: What the client can no longer do, does only with prompting, or does with significant deterioration.
- Diagnostic reasoning: Why major depressive disorder or another depressive condition best fits the presentation.
- Consistency review: Whether collateral records, family observations, and behavior during interview align.
A good legal report does more than label distress. It shows the evaluator's reasoning.
When attorneys request an evaluation, it helps to ask for specifics. Ask whether the evaluator used standardized measures, conducted a diagnostic interview, reviewed medical records, considered differential diagnoses, and addressed functional impairment in plain language. Those details often determine whether the final report reads as clinically rigorous or merely sympathetic.
Distinguishing Depression from Related Conditions
The most credible diagnosis is the one that survives comparison. In post-injury cases, depression often overlaps with PTSD, adjustment disorder with depressed mood, and the direct neurobehavioral effects of traumatic brain injury. Attorneys don't need to perform the diagnosis, but they do need to recognize why the distinctions matter.
A report that blurs these categories can weaken the case. A report that differentiates them carefully looks grounded and reliable.
Where attorneys see diagnostic confusion
PTSD and depression often appear together, but they aren't the same condition. Both can involve sleep problems, withdrawal, concentration problems, and reduced interest in activities. The difference is the driver. In PTSD, avoidance usually centers on trauma reminders, hyperarousal, intrusive memories, and threat sensitivity. In depression, withdrawal is more often driven by low energy, hopelessness, and loss of pleasure.
Adjustment disorder with depressed mood is another common alternative. This diagnosis may fit when emotional symptoms follow a stressor but don't reach the full syndrome or duration expected for major depression. In practice, adjustment disorder is often overused when the evaluator hasn't explored severity thoroughly enough.
TBI-related neurobehavioral effects create a separate challenge. A client with head injury may show irritability, slowed processing, memory problems, poor initiation, or flat affect. Those signs can resemble depression. Sometimes they are depression. Sometimes they reflect neurological injury. Sometimes both are present.
For legal purposes, the quality-of-life issue is significant. In a one-year follow-up study of minor injury patients, the depressed group had quality-of-life scores 4.2 points lower than the nondepressed group after adjustment, and the type, mechanism, and severity of physical injury were not significantly associated with post-injury quality of life, indicating depression itself was the key driver of decline (one-year follow-up study of minor injury patients).
Differential diagnosis table
| Condition | Core Feature | Symptom Driver | Typical Onset |
|---|---|---|---|
| Post-injury depression | Low mood or anhedonia with broad functional decline | Loss of pleasure, hopelessness, fatigue, guilt, reduced motivation | May emerge after acute medical stabilization and continue well beyond initial recovery |
| PTSD | Re-experiencing, trauma-linked avoidance, hyperarousal | Fear response tied to trauma reminders and threat detection | Often follows a traumatic event and becomes evident when reminders persist |
| Adjustment disorder with depressed mood | Emotional response to stressor that doesn't fully meet major depressive syndrome | Distress related to life disruption, uncertainty, or role change | Usually appears after the stressor and may be more limited in scope or duration |
| TBI neurobehavioral effects | Cognitive and behavioral changes after head injury | Neurological disruption affecting attention, memory, speed, initiation, or affect | Follows head trauma and may be evident early, though some complaints persist into recovery |
A thorough differential often requires a more detailed cognitive workup. When head injury is in the record, attorneys should know when to seek a comprehensive neuropsychological evaluation for diagnostic clarification.
The diagnosis becomes stronger when the evaluator explains not only why depression fits, but why the other plausible explanations fit less well.
That distinction matters especially in immigration cases because the report may need to withstand close review from adjudicators who are looking for overstatement. Precision is protective. It also helps the attorney build a more coherent theory of hardship and impairment.
Evidence-Based Treatments and Impact on Prognosis
Once post injury depression is identified, the next practical question is what can improve it and what barriers may interfere. For immigration cases, treatment matters for two reasons. First, it affects functioning. Second, the ability or inability to obtain treatment can itself become part of the hardship record.
What tends to help
In practice, the most common treatments are psychotherapy, psychiatric medication, or a combination of both. Psychotherapy often focuses on restoring routine, increasing activity, challenging hopeless thinking, processing the meaning of the injury, and rebuilding a damaged sense of competence. Medication may be appropriate when symptoms are more severe, more persistent, or resistant to therapy alone.
Treatment after injury has to be realistic. A client who is in pain, unable to work, caring for children, fearful of institutions, or still involved in criminal or immigration proceedings may not be able to attend treatment consistently. That doesn't mean the condition is mild. It often means the treatment plan has to adapt to the client's circumstances.
Common treatment obstacles include:
- Language mismatch: Therapy loses value when interpretation is poor or unavailable.
- Cost and coverage problems: Even motivated clients may delay care when payment is uncertain.
- Transportation and scheduling barriers: Orthopedic limits, childcare needs, and unstable work make continuity difficult.
- Cultural framing: Some clients describe depression through body symptoms, shame, or spiritual language rather than mental health terms.
Why treatment barriers matter legally
From a legal perspective, prognosis is not a simple yes-or-no question about recovery. It turns on whether the client can access consistent care, whether symptoms already affect role functioning, and whether disruption of care would predictably worsen stability.
That matters in hardship arguments. If a client needs ongoing psychiatric follow-up, trauma-informed therapy, or coordinated care after an injury, continuity is relevant. If treatment has already been interrupted by detention, relocation, abuse, or financial instability, the report should say so.
A strong prognosis section usually addresses:
- Current level of impairment
- Expected need for continued care
- Factors that support improvement
- Factors that may prolong symptoms or destabilize functioning
- Likely effect of disrupted treatment access
Good prognosis language stays measured. It doesn't promise recovery and it doesn't assume permanent incapacity. It describes the likely course based on the client's actual presentation, current supports, and barriers. That kind of restraint tends to make the report more persuasive, not less.
Documenting Functional Impairment for USCIS
USCIS and the immigration court don't need a report that states a diagnosis. They need a report that shows what the diagnosis does. The legal force of post injury depression usually comes from functional impairment. That is where clinical findings become evidence.
This checklist visual captures the core record-building tasks:
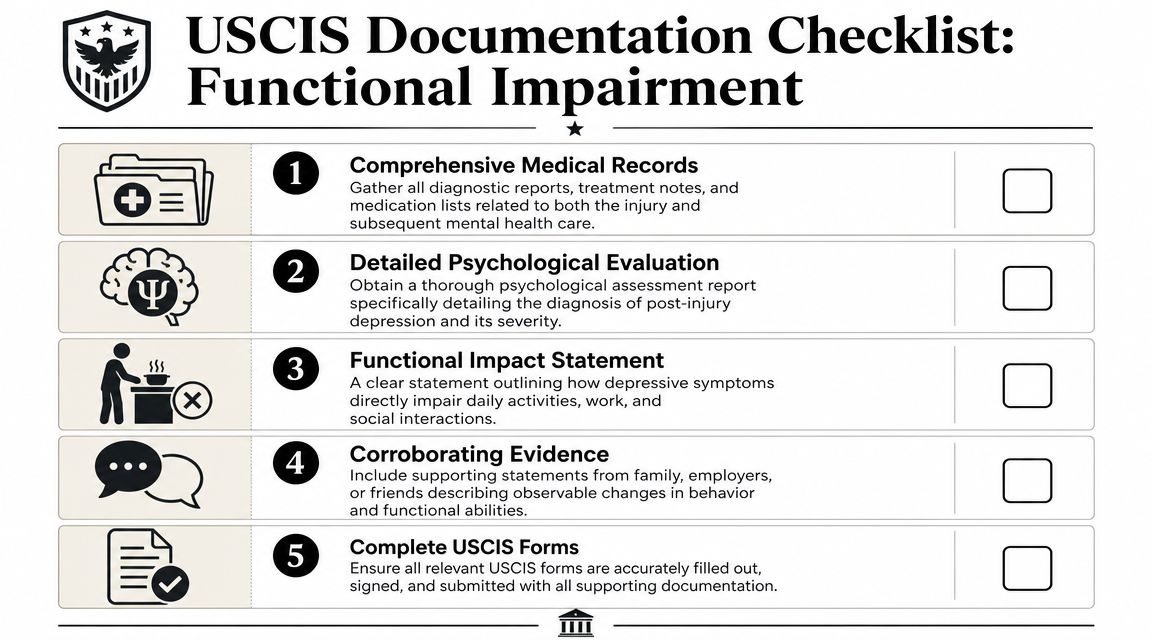
How to translate symptoms into legally useful findings
Functional impairment should be documented across concrete domains. Don't stop at “difficulty functioning.” Name the domain and describe the failure point.
A study of adults with minor injuries found that depressed patients were 8.37 times less likely to return to pre-injury activities of daily living and 2.37 times less likely to return to pre-injury work status, underscoring the connection between post-injury depression and day-to-day impairment (study on depression and return to daily functioning after minor injury).
That kind of evidence aligns with what adjudicators already understand intuitively. If depression affects dressing, hygiene, meal preparation, transportation, work attendance, concentration, and follow-through, it is no longer an abstract emotional complaint.
For immigration reports, document at least these domains:
- Daily living: bathing, dressing, cooking, cleaning, medication adherence, appointment management
- Employment or school: attendance, stamina, concentration, pace, reliability, task completion
- Family roles: childcare, supervision, emotional availability, household management
- Social functioning: withdrawal, isolation, conflict, reduced communication
- Legal participation: ability to recall events, gather documents, tolerate interviews, and assist counsel
When vocational capacity is a major issue, it can help to understand how evaluators frame limitations in a functional capacity evaluation within disability and legal settings.
Language that strengthens a report
The most persuasive reports use behavior-based descriptions. They connect symptom to consequence in one sentence.
Examples of stronger phrasing:
Instead of: “Client has severe depressive symptoms.”
Use: “Depressive symptoms interfere with the client's ability to initiate daily tasks, maintain regular attendance, and respond consistently to case-related requests.”Instead of: “Client is very sad after the injury.”
Use: “Following the injury, the client developed persistent low mood, loss of interest, social withdrawal, and reduced self-care that were not present before the event.”Instead of: “Client struggles at work.”
Use: “The client reports reduced stamina, slowed concentration, missed shifts, and difficulty completing ordinary work tasks without prompting.”
Corroboration makes these observations harder to dismiss. Useful sources include medical records, therapy notes, medication history, employer statements, school records, and declarations from relatives or friends who observed change over time.
If a symptom cannot be tied to a task, role, or daily activity, it will carry less weight in an immigration filing.
It also helps to keep causation language careful. The report should usually say the symptoms are consistent with or clinically related to the injury history and subsequent decline, rather than overstating certainty beyond the available facts. Measured language tends to survive scrutiny.
The strongest reports also address participation in the legal process itself. Depression can impair memory retrieval, reduce tolerance for emotionally loaded interviews, and make deadlines harder to meet. When that is documented clinically, what looked like inconsistency often becomes understandable functional limitation.
If you need an immigration-focused psychological evaluation that documents trauma, diagnosis, and functional impairment with clinical precision, Pro Psychological Analysis works with attorneys nationwide on U Visa, T Visa, VAWA, asylum, and hardship cases. Their reports are designed to meet legal standards while preserving the nuance that complex mental health claims require.