You're in intake with a new client. The facts are strong on paper. There was violence, threats, coercion, family separation, or a history of exploitation. But in the room, the client seems flat, detached, inconsistent, or unusually calm. They forget dates that feel central to the case. They minimize obvious abuse. They say they're “fine” and then describe weeks of sleeplessness, panic, pain, and fear of leaving the house.
That gap creates legal risk.
In mental health and immigration work, the problem often isn't that trauma is absent. It's that trauma is invisible, culturally filtered, or expressed in ways adjudicators misread. A strong psychological evaluation helps you translate a client's behavior into clinically grounded evidence. It can explain why memory is fragmented, why affect seems blunted, why someone never sought treatment, and why separation, detention, abuse, or persecution produced lasting psychiatric harm.
For attorneys, that changes the file. A declaration tells the story. A forensic evaluation gives the story clinical structure, diagnostic support, and a clear nexus to the legal standard. Used well, it doesn't decorate a case. It clarifies it.
Table of Contents
- Introduction From Legal Case to Human Story
- The Unseen Toll Migrations Impact on Mental Health
- Common Clinical Presentations and Trauma Dynamics
- The Legal Nexus Where Mental Health Evidence Matters
- Crafting an Admissible Psychological Evaluation
- Best Practices for Attorney and Evaluator Collaboration
- Partnering for Success with Pro Psychological Analysis
Introduction From Legal Case to Human Story
An immigration file usually starts with legal categories. Asylum. U visa. T visa. VAWA. Extreme hardship. The client, though, doesn't live in categories. They live in symptoms, fears, survival habits, and often a deep reluctance to discuss what happened.
That's where many otherwise strong cases weaken. The attorney sees a truthful client, but the record still has holes. The declaration may not explain why the client avoids detail, why they confuse sequence, or why they underreport abuse. A judge or officer might read those gaps as exaggeration, evasiveness, or lack of credibility when they are common trauma responses.
A client who appears emotionally flat may not be unaffected. They may be doing exactly what helped them survive.
In practice, the most useful psychological evaluations do more than attach a diagnosis to suffering. They document how trauma affects memory, functioning, behavior, and symptom expression in a way that answers legal questions. They also help when the case involves harm that isn't obvious from medical records alone, especially coercive control, cumulative fear, or the psychiatric effects of prolonged uncertainty.
Attorneys don't need to become clinicians. But they do need a working framework for knowing when mental health evidence will strengthen the case, what a proper evaluation should contain, and how to work with an evaluator so the final report is admissible, focused, and useful.
The Unseen Toll Migrations Impact on Mental Health
Migration places stress on people before departure, during transit, and after arrival. By the time a client sits in your office, you're rarely looking at a single injury. You're looking at layers.
A simple way to think about it is a backpack that keeps getting heavier. One set of stones comes from the country of origin. Another gets added during the journey. More are added after arrival through isolation, discrimination, legal uncertainty, detention, or fear of removal.
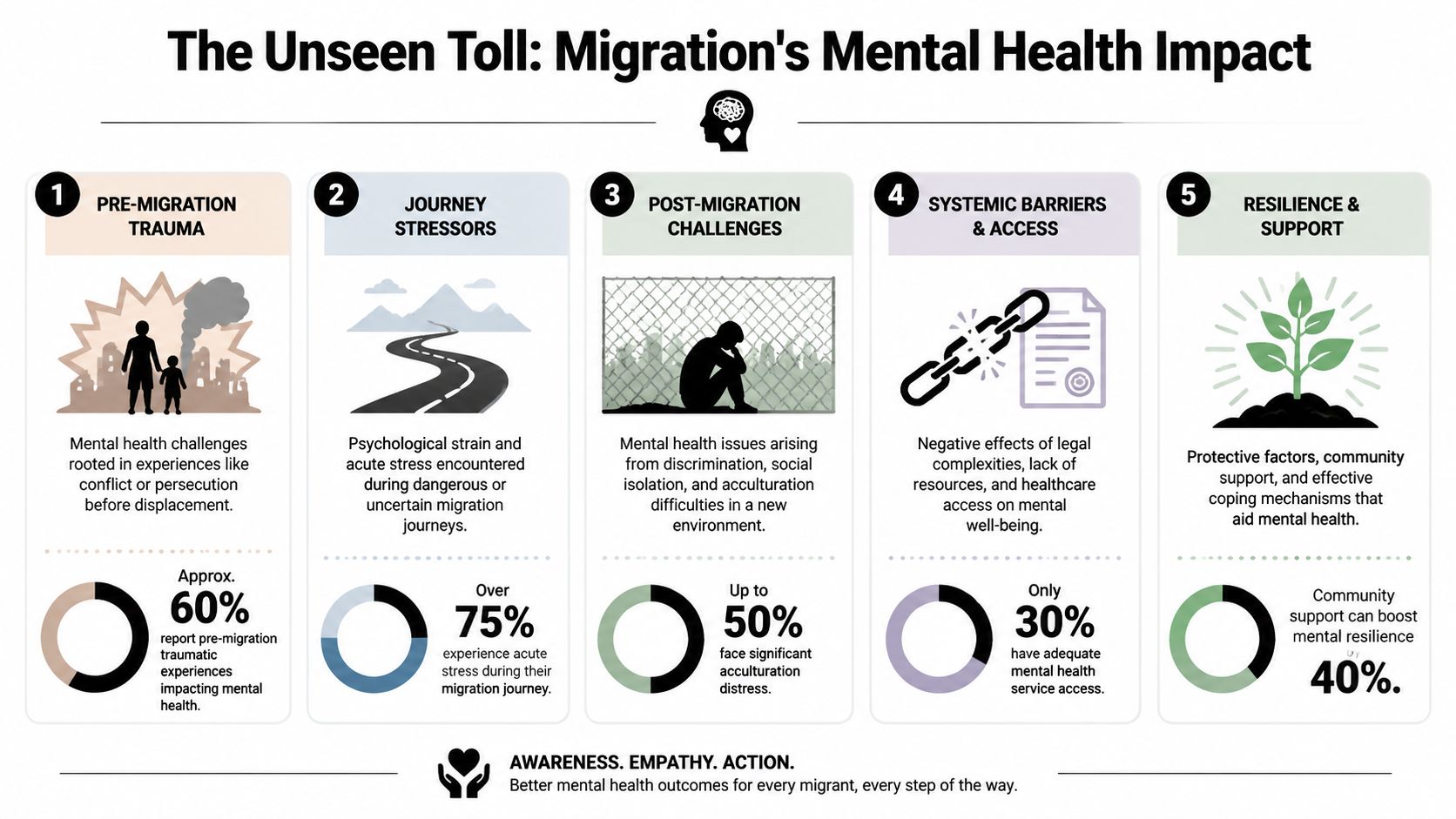
Why the timeline matters
Pre-migration stressors often include persecution, political violence, abuse, trafficking, family violence, extortion, or chronic exposure to threat. Even when the client doesn't use clinical language, these experiences can set the stage for PTSD, depression, anxiety, hypervigilance, and dissociation.
Peri-migration stressors come from the journey itself. Clients may describe danger, exploitation, deprivation, uncertainty, or separation during transit. This part of the timeline often gets underdeveloped in declarations because clients focus on the event that seems most legally important, not the cumulative burden.
Post-migration stressors are where many attorneys underestimate the psychiatric load. Acculturation stress, fear of deportation, family separation, unstable housing, inability to access care, and exposure to hostile policy environments can deepen existing symptoms or trigger new ones. In California, recent immigrants experienced a 140% surge in serious psychological distress, rising from 5% to 12% between 2015-2017 and 2019-2021, according to the UCLA Center for Health Policy Research analysis of CHIS data.
That pattern matters legally because it supports something attorneys see often. The client didn't leave trauma behind at the border. Conditions after arrival can intensify psychiatric symptoms.
What attorneys should listen for
When you build a psychosocial timeline, listen for shifts in functioning, not just dramatic incidents.
- Before migration: What was the client's baseline? School, work, caregiving, sleep, trust, concentration.
- During transit: Did symptoms change on the journey? Panic, fear, numbness, physical pain, shutdown, mistrust.
- After arrival: What happened once they were “safe”? Many clients decompensate only after immediate survival pressure drops.
Practical rule: A chronology that tracks symptom onset and worsening is often more persuasive than a chronology that only lists bad events.
For mental health and immigration cases, chronology is strategy. It helps the evaluator identify causation, and it helps you show why the client's current presentation fits the history rather than undermines it.
Common Clinical Presentations and Trauma Dynamics
A traumatized client won't always present as visibly traumatized. Some cry easily. Others laugh when discussing assault. Some can recount a peripheral detail with precision but can't sequence the central event. None of that is unusual.

Trauma rarely looks neat
The clinical presentations attorneys encounter most often include PTSD symptoms, depressive symptoms, anxiety, panic, dissociation, traumatic grief, and somatic distress. But the visible signs are usually behavioral, not diagnostic.
You may see:
- Emotional numbing: The client sounds flat or detached when discussing severe events.
- Fragmented recall: The story has sensory detail but weak sequence or unclear timing.
- Avoidance: The client minimizes, redirects, or says they don't want to think about it.
- Somatic expression: Headaches, chest pain, stomach distress, fatigue, or generalized pain become the primary complaint.
- Hyperarousal: Startle, vigilance, sleep disturbance, irritability, or fear in public spaces.
These patterns can create credibility concerns if they aren't interpreted clinically. They can also vary across culture, language, gender, and community norms. Some clients don't use terms like trauma, anxiety, or depression. They may describe “pressure,” “nerves,” “sadness,” “thinking too much,” or bodily pain. A good evaluator doesn't force Western phrasing onto the client. The evaluator translates the client's actual report into clinically defensible language.
A quick visual shorthand can help attorneys discuss this issue with staff and clients. The brain and symptom icon reference is useful for explaining that behavior, memory, and affect can all shift under chronic threat.
{kind=link}
Why no treatment history may help explain the case
One of the most common attorney concerns is, “There are no mental health records. Will that hurt us?” Usually, no. Often, it helps explain the barriers the client has lived under.
Research summarized in Immigrant access to mental health services found that immigrants with psychiatric diagnoses use services at rates of 5-40%, compared with 59-71% among U.S.-born adults. That same body of research supports a key forensic point: lack of prior treatment is not proof of wellness. It may reflect language barriers, legal status concerns, stigma, cost, limited transportation, fear of institutions, or the fact that survival came before treatment.
When a client has no therapy records, don't assume you have an evidentiary weakness. Ask why treatment was inaccessible, unacceptable, or unsafe.
That issue is especially important in immigration cases because adjudicators may expect medical corroboration. A forensic evaluation can document untreated symptoms, explain delayed help-seeking, and distinguish symptom onset from treatment initiation.
A short explainer can also help teams calibrate what trauma looks like in real conversation:
What doesn't work is pushing clients to produce a “clean” trauma narrative too early. What works is careful interviewing, allowing culturally shaped language, and letting a qualified evaluator connect symptoms, behavior, and chronology.
The Legal Nexus Where Mental Health Evidence Matters
Not every case needs a psychological evaluation. But when the legal claim depends on proving harm, fear, coercion, abuse dynamics, or the psychiatric consequences of separation, mental health evidence can become central rather than supplemental.
In asylum-related contexts, one of the most useful functions of an evaluation is documenting how trauma maps onto current diagnosis and functioning. That link matters because restrictive systems themselves can worsen psychiatric injury. A 2024 meta-analysis summarized by the U.S. Committee for Refugees and Immigrants found that over one-third of people in indefinite asylum-waiting situations suffer from PTSD, over one-third from anxiety disorders, and approximately half from depression.
Role of psychological evaluations by case type
| Case Type | Primary Legal Question Addressed by Evaluation | Key Clinical Focus |
|---|---|---|
| Asylum | Does the client show clinical effects consistent with past persecution or ongoing fear? | Trauma history, PTSD symptoms, depression, anxiety, memory fragmentation, functional impairment |
| T Visa | Did trafficking produce substantial psychological harm? | Coercion, captivity dynamics, fear conditioning, trauma symptoms, shame, dissociation |
| U Visa | Did the qualifying crime result in substantial mental abuse? | Post-crime symptoms, panic, sleep disturbance, avoidance, depressive symptoms, safety concerns |
| VAWA | Did battery or extreme cruelty create clinically significant psychological impact? | Coercive control, traumatic bonding, chronic fear, self-blame, depression, PTSD, helplessness |
| Extreme Hardship Waiver | Would separation or relocation create exceptional psychological hardship to the qualifying relative? | Baseline functioning, dependency, caregiving burden, psychiatric vulnerability, likely deterioration under separation |
The same tool serves different strategic purposes depending on the case. In asylum, the report often explains persecution's psychiatric footprint and why testimony may appear inconsistent without being false. In T and U matters, the report helps document substantial harm. In VAWA, it can clarify coercive control when police reports or medical records are limited. In hardship cases, the focus usually shifts to projected impact on a qualifying relative.
When an evaluation adds the most value
An evaluation is often worth prioritizing when the file includes one or more of these problems:
- Credibility vulnerability: Flat affect, inconsistent sequencing, minimization, or avoidance.
- Invisible harm: Abuse, coercion, or fear that didn't generate extensive external records.
- Barrier-to-care history: No treatment records despite strong symptom presentation.
- Nexus questions: You need a clinician to connect symptoms to persecution, trafficking, abuse, or likely hardship.
- Functional decline: Work, sleep, caregiving, concentration, school, or daily functioning have changed.
A weak use of mental health evidence is attaching a generic letter that says the client is anxious and should remain in the United States. A strong use is presenting a methodical forensic report that answers the legal question embedded in the case.
Crafting an Admissible Psychological Evaluation
An admissible psychological evaluation does more than document distress. It gives the court or adjudicator a reliable clinical basis for a legal conclusion.
That requires forensic method. A report written for immigration proceedings should show how the evaluator gathered information, tested competing explanations, and connected the findings to the specific issue in dispute. The published discussion of that gap in immigration mental health practice makes the problem clear. Attorneys often receive letters that sound supportive but do little evidentiary work.
What separates a forensic report from a support letter
A treatment provider may know the client well and still produce a weak immigration exhibit. The problem is usually not sincerity. It is fit. Treatment records are built for care, symptom tracking, and risk management. A forensic immigration report is built for evidence.
A usable evaluation usually includes:
- Clinical interview: A detailed psychosocial history, trauma history, current symptom review, and functional assessment.
- Record review: Relevant declarations, affidavits, police reports, medical records, school records, or prior filings, if available.
- Diagnostic reasoning: A clear explanation of why the diagnosis fits the reported symptoms, observed presentation, and available records.
- Nexus analysis: A direct connection between the clinical findings and the legal question.
- Professional method: Objective tone, informed consent, defined forensic role, and clear limits on the opinion.
Those elements matter because admissibility and persuasive value rise or fall on method. A short letter that states the client has anxiety and should stay in the United States rarely helps. A structured report that explains symptoms, impairment, causation, and limits of the opinion can.
What USCIS and the court need to see
Judges and adjudicators do not need dramatic language. They need clinical reasoning they can follow.
The strongest reports usually do five things well:
Separate sources of information clearly.
The report distinguishes the client's statements, collateral records, behavioral observations, and the evaluator's opinions.Address inconsistencies directly.
If the timeline shifts, memory is fragmented, or disclosure is delayed, the report explains whether trauma, dissociation, shame, fear, or cognitive symptoms may account for that pattern.Describe functional impairment, not just symptoms.
Diagnostic labels alone do not carry a case. The report should explain how symptoms affect sleep, concentration, work, parenting, schooling, social contact, or daily tasks.Answer the legal question presented.
In hardship cases, that often means projected psychiatric deterioration, treatment disruption, or caregiving impact. In VAWA matters, it may mean documenting coercive control, trauma effects, and why corroborating records are limited.Stay readable.
Dense jargon and sweeping conclusions create problems. Plain clinical language is more persuasive.
Case strategy note: The strongest evaluation anticipates the question that will decide the case and answers it with clinical support.
If you're vetting evaluators, ask for a redacted sample. Review the structure, the reasoning, and the restraint. Strong evaluators explain what they know, how they know it, and where the limits are. Pro Psychological Analysis is one example of a service focused on immigration-specific psychological evaluations and court-ready reporting.
Best Practices for Attorney and Evaluator Collaboration
Most problems with psychological evidence start upstream. The evaluator receives a rushed referral, limited records, no explanation of the legal standard, and a deadline that should have been raised two weeks earlier. Then everyone hopes the report will somehow answer questions no one framed.
That's preventable.
What to send with the referral
Give the evaluator a focused packet, not a data dump. The packet should help the clinician understand the legal theory and the evidentiary gaps.
Include:
- Case posture: Filing type, forum, deadline, and whether testimony, declaration, or prior filings already exist.
- Target legal issue: What exactly should the report help establish? Past persecution, substantial harm, extreme cruelty, hardship, credibility support, or another point.
- Core records: Declaration drafts, prior statements, police reports, medical records, country-condition materials if relevant to context, and any prior psychological records.
- Practical concerns: Interpreter needs, literacy issues, safety concerns, contact constraints, and whether the client has difficulty discussing specific topics.
A concise attorney memo is often more helpful than a long email thread. Spell out the questions you want answered.
Ethical guardrails that protect the case
The evaluator's role isn't to become part of the legal team. It's to provide an objective clinical opinion. That objectivity is one reason the report has weight.
Key guardrails include:
- Confidentiality: Use HIPAA-compliant systems and make sure the client understands who will receive the report.
- Role clarity: Treating therapists and forensic evaluators serve different functions. Combining those roles can create avoidable problems.
- Interpreter competence: Use qualified interpreters when needed, and document interpreter involvement.
- No coaching: Attorneys should prepare clients for process, not script symptoms or expected diagnoses.
- Time for accuracy: Last-minute evaluations are sometimes unavoidable, but rushed interviews increase the risk of omissions and weaker analysis.
Good collaboration means the attorney supplies the legal lens, and the evaluator supplies the clinical one. Neither should try to replace the other.
When that partnership works, the report becomes far more precise. It addresses the case you're filing, not a generic version of immigrant distress.
Partnering for Success with Pro Psychological Analysis
The practical lesson in mental health and immigration cases is simple. The strongest evaluations do more than confirm that a client is suffering. They explain how the suffering developed, how it appears clinically, why it may not look the way non-clinicians expect, and how it connects to the legal standard in front of USCIS or the immigration court.
That requires a specific kind of work. It requires forensic thinking, careful interviewing, trauma literacy, cultural responsiveness, clean documentation, and a process that fits legal deadlines. It also requires a team that knows how to collaborate with counsel without drifting into advocacy language that weakens the report.
For attorneys who need that type of support, learn more about the Pro Psychological Analysis team. The practice provides immigration-focused psychological evaluations for asylum, T visa, U visa, VAWA, and hardship matters, with HIPAA-compliant processes, virtual options, and reports designed for legal use.
{kind=link}
A good evaluation won't fix a weak legal theory. But in the right case, it can turn a misunderstood presentation into credible evidence, convert invisible harm into documented injury, and give adjudicators a clinically grounded reason to understand what happened to your client and why it matters now.
If your case needs mental health evidence that is clear, ethical, and legally useful, Pro Psychological Analysis works with attorneys to produce immigration-focused psychological evaluations that document trauma, diagnosis, and nexus in a form built for USCIS and court review.