A client sits across from counsel and says she can't sleep, startles at hallway noise, forgets dates, has stomach pain, and goes numb when asked about the abuse. On paper, that can look inconsistent. In practice, it often reflects one coherent clinical picture.
Immigration attorneys see this problem constantly. A survivor's history is real, but the presentation is fragmented. One part sounds psychiatric. Another sounds medical. Another looks like poor memory or evasiveness. If the case record treats those pieces as unrelated complaints, the legal narrative weakens.
Nervous system dysregulation gives those facts a clinically grounded frame. It connects hypervigilance, insomnia, digestive disturbance, chronic pain, brain fog, emotional volatility, shutdown, and sensory sensitivity to the same underlying problem. The person's stress response system is no longer returning to baseline in an ordinary way after trauma.
That matters in immigration cases because adjudicators don't just evaluate what happened. They evaluate whether the evidence credibly shows lasting harm, coercion, fear conditioning, functional impairment, and trauma-consistent presentation. When a clinician documents dysregulation carefully, the report does more than repeat symptoms. It translates diffuse suffering into physiological evidence.
For Asylum, T, U, and VAWA matters, that shift is often decisive. It helps explain why a client couldn't leave, couldn't disclose earlier, can't recall events linearly, or continues to react as if danger is present even when the threat has ended. It also helps attorneys argue that the record shows more than distress. It shows a body and mind altered by prolonged threat exposure.
Table of Contents
- Introduction When Trauma Symptoms Defy Easy Description
- The Body's Alarm System The Autonomic Nervous System
- How Trauma Hijacks the Nervous System
- Assessment Methods and Screening Tools
- Documenting Dysregulation for USCIS and Immigration Court
- How PPA Evaluations Meet Evidentiary Standards
- Conclusion From Clinical Finding to Legal Cornerstone
Introduction When Trauma Symptoms Defy Easy Description
An attorney may have a declaration that reads clearly, yet the client in interview seems scattered, flat, agitated, or confused. She reports migraines, poor sleep, stomach distress, panic, and memory gaps. He describes constant scanning of exits, irritability, numbness, and episodes of “blanking out” when discussing the trafficking. None of those facts are trivial. Together, they often describe a stress system that has lost flexibility.
The legal risk is obvious. Without a unifying framework, the record can look messy. Medical symptoms get separated from psychological symptoms. Memory problems get mistaken for credibility problems. A survivor's inability to narrate events in a calm, chronological way can be misunderstood as inconsistency rather than a trauma-linked response pattern.
Nervous system dysregulation solves that problem when used correctly. It ties the client's presentation to autonomic functioning, meaning the body systems that regulate heart rate, breathing, digestion, arousal, and recovery after stress. Instead of asking whether every symptom fits neatly into one label, the evaluator asks a better question: do these symptoms reflect a body that remains organized around threat?
Practical rule: If the client's symptoms span body, mood, cognition, sleep, and behavior, don't assume the case is diffuse. It may be highly coherent at the physiological level.
For immigration practice, that distinction matters because many forms of relief turn on the effects of persecution, abuse, coercion, or qualifying victimization. A well-prepared evaluation doesn't merely state that the person feels anxious. It documents how trauma altered baseline functioning, how that change appears in daily life, and why the pattern is clinically consistent with the claimed history.
Attorneys don't need to become neurobiology specialists. They do need to recognize when a client's presentation is best understood as trauma-driven dysregulation rather than poor cooperation, weak recollection, or generalized stress.
The Body's Alarm System The Autonomic Nervous System
The autonomic nervous system runs much of what clients don't consciously control. It regulates heart rate, breathing, digestion, sleep, and stress responses. In plain terms, it is the body's alarm-and-recovery system.
What the system does
The simplest analogy is a car. The sympathetic nervous system is the gas pedal. It mobilizes the body for danger. The parasympathetic nervous system is the brake. It supports rest, recovery, and return to baseline.
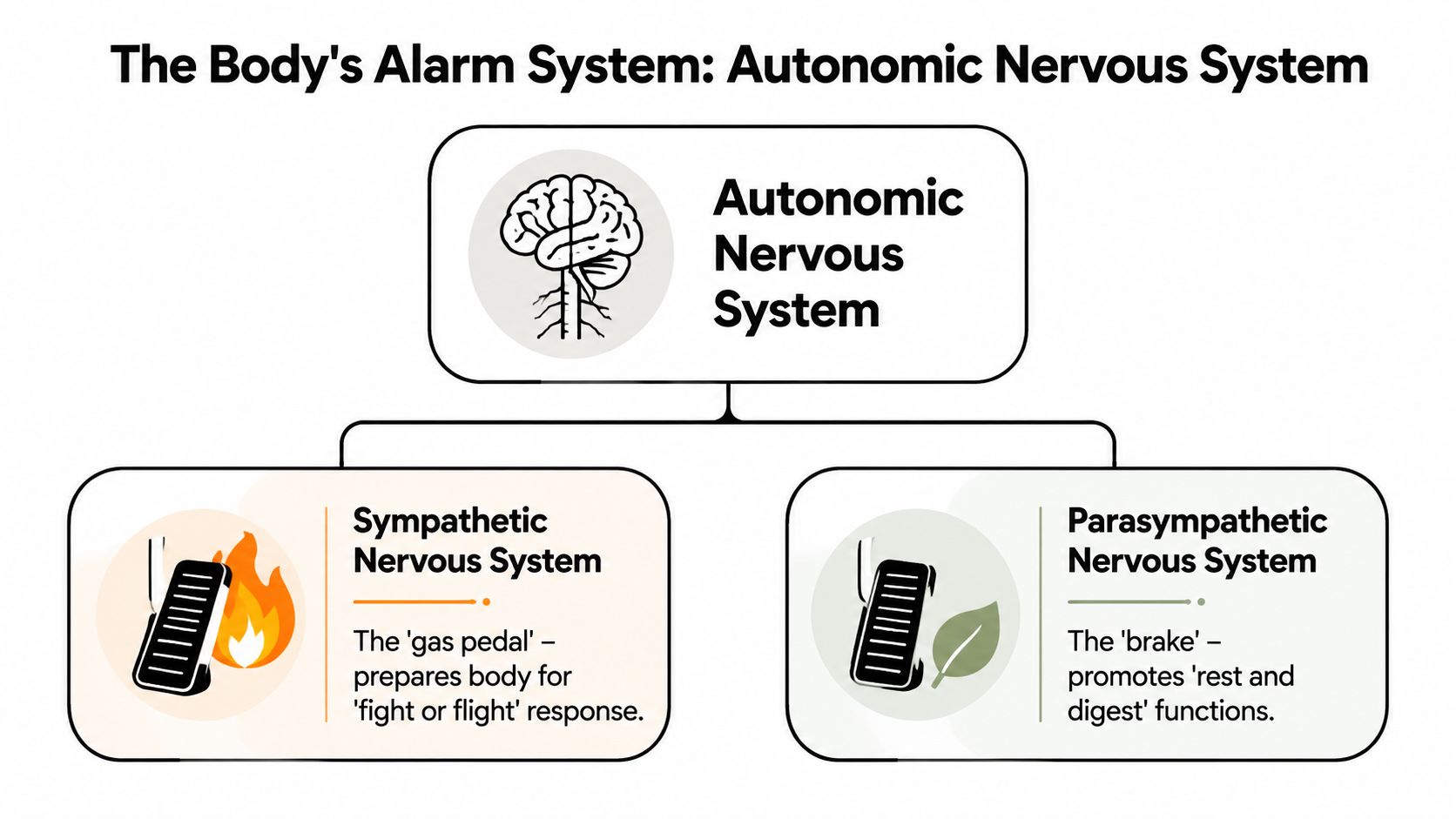
That system works well when it is flexible. The body speeds up when there is danger, then slows down when danger passes. Nervous system dysregulation appears when that flexibility is lost. The gas pedal stays pressed too long, or the brake doesn't engage effectively. Sometimes the reverse happens. The system overcorrects into shutdown, collapse, or disconnection.
A clinically useful summary from Healthline's review of nervous system dysregulation is that dysregulation reflects altered autonomic control, where the sympathetic branch remains excessively activated or the parasympathetic branch fails to restore balance. The result is measurable downstream effects in heart rate, breathing, digestion, sleep, and pain sensitivity.
What dysregulation looks like clinically
For attorneys, this is the important translation: the client is not merely “emotional.” The client may be physiologically unable to settle. That can show up as:
- Hyperarousal signs like insomnia, startle, rapid breathing, agitation, muscle tension, and hypervigilance
- Hypoarousal signs like numbness, dissociation, slowed speech, exhaustion, blankness, and collapse
- Mixed patterns where the client shifts between panic and shutdown, often during the same interview process
The body can remain organized around survival long after the threat environment changes.
That is why some survivors appear guarded in one interview and emotionally flat in another. It is also why legal professionals should be cautious about reading calmness as wellness or disorganization as deception.
A good evaluation links these patterns to functioning. Is the client sleeping poorly, unable to concentrate, avoiding reminders, struggling with digestion, or reacting intensely to ordinary sensory cues? Those observations strengthen the record because they show consequences that are consistent with trauma physiology, not just subjective suffering.
How Trauma Hijacks the Nervous System
Trauma doesn't only produce fear memories. It can recalibrate the body's stress response so the person keeps reacting as if the threat is still active.

Why the threat response doesn't simply turn off
Abuse, trafficking, captivity, coercive control, persecution, and repeated interpersonal violence teach the nervous system a brutal lesson. Safety is uncertain. Neutral cues may not be neutral. Rest may not be safe. Disclosure may carry danger.
A systematic review on HPA-axis vulnerability found that early life adversity and later stress exposures shape cortisol and stress-reactivity patterns, increasing the likelihood of persistent hyperarousal or blunted responding. In legal terms, that helps explain why clients may remain physiologically reactive long after the original threat has passed.
Clinicians often use the window of tolerance model. Inside the window, a person can think, feel, recall, and respond with relative stability. Above the window, the person moves toward hyperarousal. Below it, the person drops into hypoarousal.
The window of tolerance in legal interviews
Hyperarousal often looks easier to recognize. The client cries, trembles, startles, scans the room, or reports racing thoughts and sleeplessness. Hypoarousal is easier to miss. The client becomes monotone, detached, confused, slowed, or unable to access detail. Both states can be trauma-consistent.
For attorneys, that has immediate consequences:
- Disclosure may be delayed because discussing the event triggers the same alarm response that helped the person survive.
- Memory may be uneven because threat-state encoding doesn't always produce neat chronology.
- Affect may not match expectation because shutdown can flatten emotional expression.
- Avoidance may be protective rather than oppositional.
A useful primer on this broader trauma pattern appears in PPA's article on understanding complex trauma.
After a client has moved outside the window of tolerance, more questioning often produces less reliable information, not more. That is a practical trade-off attorneys should take seriously. Pressing for detail in a dysregulated state can worsen fragmentation, increase shame, and reduce coherence.
A short visual explanation can help orient teams that work with survivors:
The mistake is to assume that if the threat is over, the body should behave as though it knows that. Often, it doesn't.
Assessment Methods and Screening Tools
A credible opinion about nervous system dysregulation doesn't come from intuition. It comes from a methodical assessment that integrates narrative history, symptom pattern, clinical observation, and standardized tools.
Start with a structured clinical interview
The interview remains central because dysregulation often appears in the connections between symptoms. The evaluator asks about sleep, startle, concentration, somatic complaints, dissociation, avoidance, sensory sensitivity, pain, gastrointestinal disruption, and what happens in the body when trauma reminders appear.
The symptom range matters. According to the PubMed-indexed discussion of autonomic dysregulation and related symptom profiles, common signs can include chronic anxiety, mood swings, sleep disturbance, digestive issues, chronic pain, sensory sensitivity, hypervigilance, and brain fog. That breadth is exactly why a narrow interview often misses the full picture.
A structured method also reduces forensic risk. It creates a clear record of onset, duration, triggers, current impairment, and trauma linkage. For attorneys who want a useful overview of that process, PPA has a concise explanation of the structured interview in psychological evaluations.
Common tools for assessing trauma and dysregulation
No single measure captures the full phenomenon. Strong evaluations combine tools based on the referral question and the client's presentation.
| Tool Name | What It Measures | Relevance for Immigration Cases |
|---|---|---|
| PTSD symptom inventories | Trauma-related intrusion, avoidance, arousal, negative mood and cognition | Helps organize symptoms tied to persecution, assault, trafficking, or domestic violence |
| Dissociation measures | Detachment, depersonalization, derealization, memory disruption | Useful when the client reports blankness, numbness, time loss, or fragmented recall |
| Depression and anxiety scales | Mood symptoms, generalized distress, physiological anxiety | Clarifies severity and comorbidity without reducing the case to one diagnosis |
| Somatic symptom measures | Physical distress linked to stress activation | Supports documentation when the client presents with pain, gastrointestinal distress, fatigue, or sleep disturbance |
| Functional impairment measures | Effects on work, parenting, concentration, and daily living | Connects clinical findings to real-world hardship and credibility concerns |
| Clinical mental status examination | Behavior, affect, thought process, attention, memory, orientation | Provides observed data that can corroborate dysregulated presentation during the evaluation |
What weak assessments get wrong
Some reports fail because they collapse everything into a generic conclusion like “client is traumatized.” Others list diagnoses without showing how the evaluator reached them. In immigration matters, that isn't enough.
Forensic priority: The report should show the chain of reasoning, not just the endpoint.
Weak assessments also ignore body-based symptoms. That is a major loss. If a client reports disturbed sleep, digestive problems, chronic pain, sensory overload, and exaggerated startle, those facts can corroborate a trauma-related physiological pattern. Leaving them out makes the record thinner than it should be.
The most persuasive reports do something more difficult and more useful. They integrate psychometrics, behavioral observations, trauma history, and functional consequences into one clinically coherent formulation.
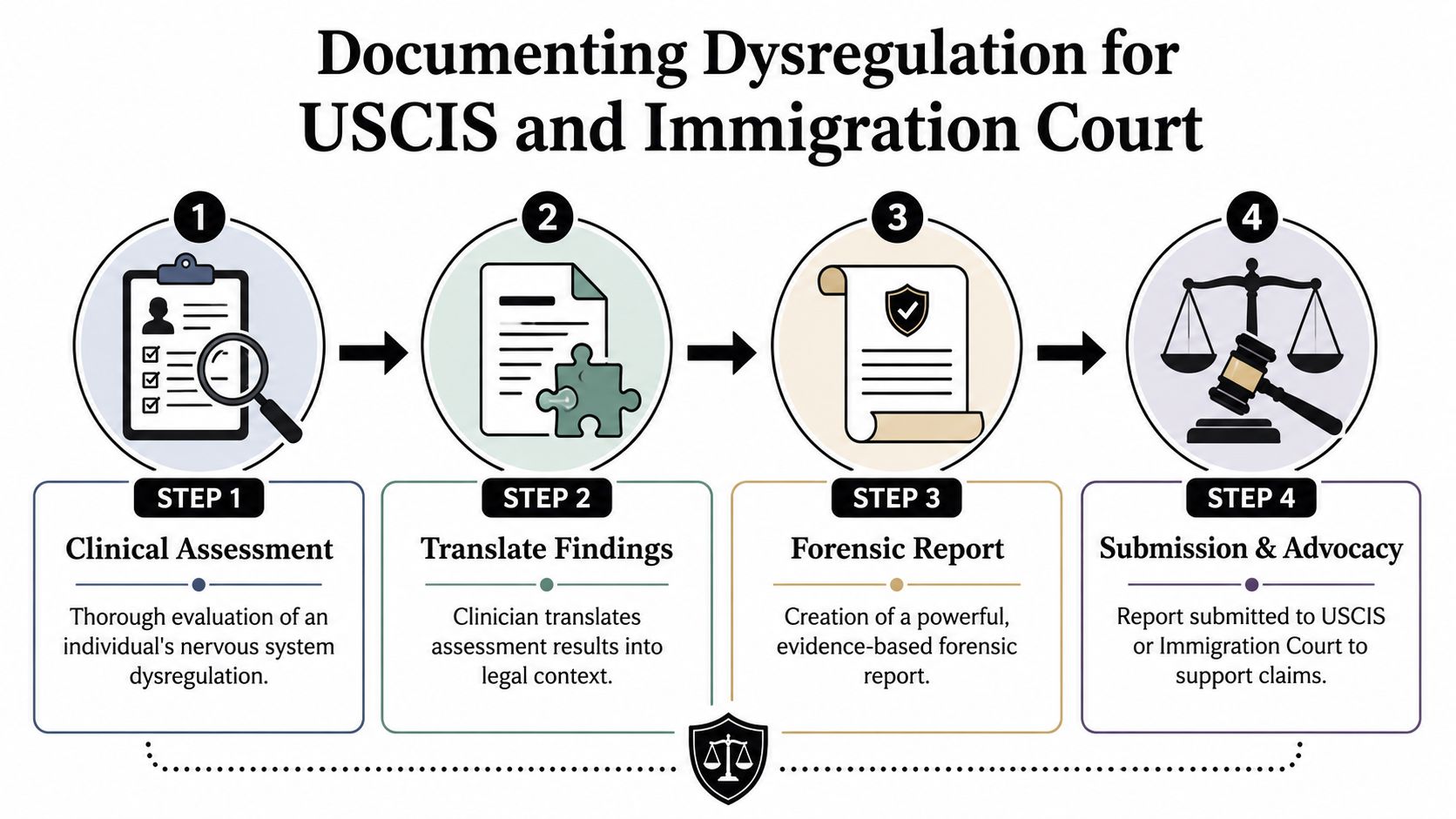
Documenting Dysregulation for USCIS and Immigration Court
The legal value of nervous system dysregulation depends on documentation. If the report uses vague wellness language, it won't help much. If it translates clinical findings into a disciplined forensic opinion, it can substantially strengthen the case record.
What belongs in a defensible report
A defensible report identifies the relevant trauma exposure, describes the symptom pattern, explains why that pattern is consistent with dysregulation, and ties the findings to functional impairment. The report should also distinguish observations from client self-report and explain how standardized measures informed the opinion.
Attorneys should look for several features:
- Trauma linkage that connects symptoms to persecution, coercive control, trafficking, sexual violence, or qualifying victimization
- Physiological detail such as insomnia, startle, panic physiology, gastrointestinal disturbance, pain amplification, or shutdown states
- Behavioral observations including guardedness, distractibility, dissociation, freezing, tearfulness, scanning, or flattened affect
- Functional consequences affecting memory retrieval, concentration, work, relationships, parenting, or participation in legal proceedings
- Clinical reasoning that explains why the presentation supports the stated conclusions
A historical point gives this framework real evidentiary force. News-Medical's summary of autonomic research notes that a 2013 PubMed-indexed study reported that autonomic dysregulation predicts cardiovascular disease and diabetes, reinforcing that dysregulation is not merely a subjective wellness concept but a measurable physiological state with downstream health consequences.
That matters in court filings and affidavits because it supports a simple proposition: the clinician is not rebranding distress with fashionable language. The clinician is describing a recognized pattern of altered stress regulation with observable effects.
For lawyers working with supporting records, PPA's overview of medical documentation in immigration cases is a useful companion resource.
How dysregulation supports specific forms of relief
The application differs by case type.
In Asylum cases, dysregulation can corroborate the enduring impact of persecution or torture and explain fragmented recall, fear responses, and difficulty narrating traumatic events. In T visa matters, it can help show the effects of trafficking, coercion, captivity, and trauma bonding. In U visa cases, it can support substantial abuse and ongoing impairment after qualifying criminal victimization. In VAWA cases, it can help demonstrate the psychological and physiological effects of battering, intimidation, surveillance, sexual abuse, and coercive control.
The strongest reports don't just state that trauma occurred. They show how the body still bears its imprint.
A frequent mistake is overclaiming. Dysregulation doesn't prove every allegation by itself. It does something narrower and very powerful. It provides corroborative clinical evidence that the client's current functioning is consistent with prolonged threat exposure and trauma-related impairment.
That is often exactly what USCIS officers, immigration judges, and opposing parties need to see.
How PPA Evaluations Meet Evidentiary Standards
Strong immigration evaluations have to do two jobs at once. They must be clinically sound, and they must be usable by counsel.
Clinical rigor matters more than wellness language
Many reports commonly fail. They borrow popular terms about regulation, vagal tone, grounding, or self-care without showing how any of that supports a forensic conclusion. The result sounds compassionate but not especially admissible.
That concern tracks the broader literature. The Universal Health Fellowship discussion of nervous system dysregulation notes a central challenge: separating evidence-informed analysis from generic advice. That distinction matters even more in legal settings, where the evaluator must explain not only what symptoms exist, but why the conclusions follow from the assessment.
In practice, a rigorous evaluation does several things well:
- It gathers a detailed trauma narrative without forcing artificial chronology.
- It uses validated instruments rather than relying on impression alone.
- It documents physiological, cognitive, and emotional symptoms together.
- It explains inconsistencies clinically when they are trauma-consistent.
- It avoids exaggerated claims the data can't support.
What attorneys need from the final report
From a legal strategy standpoint, the best report is readable, specific, and tethered to the relief sought. It should help counsel answer practical questions. Why didn't the client disclose sooner? Why is memory fragmented? Why does the client remain fearful in apparently safe settings? Why do physical symptoms matter to the claim?
A useful report also respects trade-offs. Not every symptom needs equal attention. Not every diagnosis is legally important. The evaluator should prioritize findings that illuminate persecution, abuse dynamics, coercion, sustained fear, and functional impairment.
When that work is done carefully, the report becomes more than a clinical summary. It becomes a bridge between trauma physiology and legal proof.
Conclusion From Clinical Finding to Legal Cornerstone
Nervous system dysregulation belongs in immigration practice because it explains a pattern attorneys already see. The client who can't sleep, startles easily, forgets details, goes blank under stress, and develops pain or digestive disruption after trauma is not presenting with random complaints. The client may be showing the ongoing effects of a stress system that no longer resets normally.
That clinical framing has legal value. It helps decision-makers understand why trauma survivors often present in fragmented, nonlinear, body-based ways. It helps separate credibility concerns from trauma effects. It converts a vague story of suffering into a documented account of physiological harm.
For Asylum, T, U, and VAWA matters, that shift can be substantial. A disciplined psychological evaluation can connect the dots between the underlying trauma, the present symptom pattern, and the person's impaired functioning in daily life and during legal proceedings. That is often what makes the record persuasive.
Attorneys don't need broad claims. They need careful ones. When nervous system dysregulation is assessed methodically and documented with forensic discipline, it can serve as a cornerstone of proof rather than a passing clinical phrase.
If you need an immigration psychological evaluation that translates trauma, abuse dynamics, and nervous system dysregulation into clear, evidence-based findings for USCIS or immigration court, Pro Psychological Analysis provides specialized assessments for Asylum, T visa, U visa, VAWA, and hardship cases. Their reports are designed to align with legal strategy, document clinically relevant symptoms with rigor, and present conclusions in a form attorneys can use.