Only 31% of Black adults with mental illness receive treatment annually, compared to 48% of white adults according to Western Youth Services on BIPOC mental health disparities and access to care. For immigration lawyers, that isn't just a public health statistic. It's a case development issue.
When a client has learned to survive without formal care, legal teams often misread the consequences. A fragmented timeline may look evasive. Flat affect may look indifferent. Delayed disclosure may look inconsistent. In practice, those patterns often reflect trauma, distrust, stigma, or prior experiences with systems that didn't protect them.
That is why bipoc mental health month matters inside an immigration practice. July is an opportunity to improve how your team interviews clients, identifies when a psychological evaluation may help, and builds records that reflect the full impact of persecution, abuse, trafficking, detention, and chronic discrimination. The month honors Bebe Moore Campbell National Minority Mental Health Awareness Month, observed every July and formally designated by the U.S. House of Representatives in 2008 through House Resolution 978, as described by North Range Behavioral Health's overview of BIPOC Mental Health Month.
For attorneys handling asylum, VAWA, T visa, and U visa matters, this isn't symbolic programming. It's a practical shift in how you gather testimony, document impairment, and support clients whose trauma doesn't present in neat chronological order.
Table of Contents
- Why BIPOC Mental Health Month Matters for Your Practice
- Understanding the Data on Mental Health Disparities
- The Compounded Trauma of BIPOC Immigrants
- Adopting a Trauma-Informed Legal Framework
- Actionable Steps for Your Firm This July
- Building a Supportive Ecosystem Beyond Your Firm
- From Awareness to Action A Commitment to Your Clients
Why BIPOC Mental Health Month Matters for Your Practice
Most firms treat mental health awareness as a community relations topic. Immigration practice can't afford that separation. Mental health directly affects memory, disclosure, client trust, interview pacing, and the quality of declarations.
BIPOC Mental Health Month exists because communities of color have faced persistent disparities in recognition, access, and quality of care. In legal practice, those disparities show up as delayed treatment, undocumented symptoms, and narratives that appear incomplete until someone asks better questions. A lawyer may have the correct legal theory and still miss the clinical reality shaping the testimony.
The legal consequences of overlooking mental health
A client who has survived repeated trauma may not tell their story in a linear way. They may remember sensory details but not dates. They may minimize abuse because they've normalized it. They may omit the event that matters most until trust has been built over several meetings.
Practical rule: If a client's presentation seems inconsistent, first ask what trauma, stigma, or fear might explain the pattern before assuming credibility problems.
BIPOC clients often carry another layer. They may distrust institutions, avoid disclosure because of cultural stigma, or interpret symptoms through community-specific language rather than diagnostic terms. Attorneys who understand that dynamic usually gather better evidence and avoid preventable missteps, especially in cases involving persecution, coercive control, trafficking, family violence, or severe hardship.
Why July should change your intake habits
The value of bipoc mental health month is that it gives firms a concrete moment to audit process. Not mission statements. Process.
Use July to review whether your staff:
- Prepares clients for difficult interviews instead of starting with the most painful facts
- Knows when to pause rather than pushing through visible dysregulation
- Understands referral thresholds for psychological evaluation
- Explains confidentiality clearly so clients know what is and isn't shared
The firms that do this well don't just look more compassionate. They build cleaner records, get more accurate trauma histories, and reduce the risk that a client's distress will be mistaken for unreliability.
Understanding the Data on Mental Health Disparities
The data matters because it gives legal teams context for behavior that might otherwise be misread. If your client population faces higher burdens and lower treatment access, then untreated symptoms shouldn't be treated as unusual. They should be expected and planned for.
What the numbers show
According to Pathlight Behavioral Health's BIPOC mental health facts and statistics, 17.3% of non-Hispanic Black or African American adults experience mental illness annually, while mixed or multiracial adults face the highest rate at 35.8%. The same source notes that Black Americans below the poverty line are twice as likely to report serious psychological distress, and that suicide is the second leading cause of death for ages 10 to 14 and the third leading cause of death for ages 15 to 24.
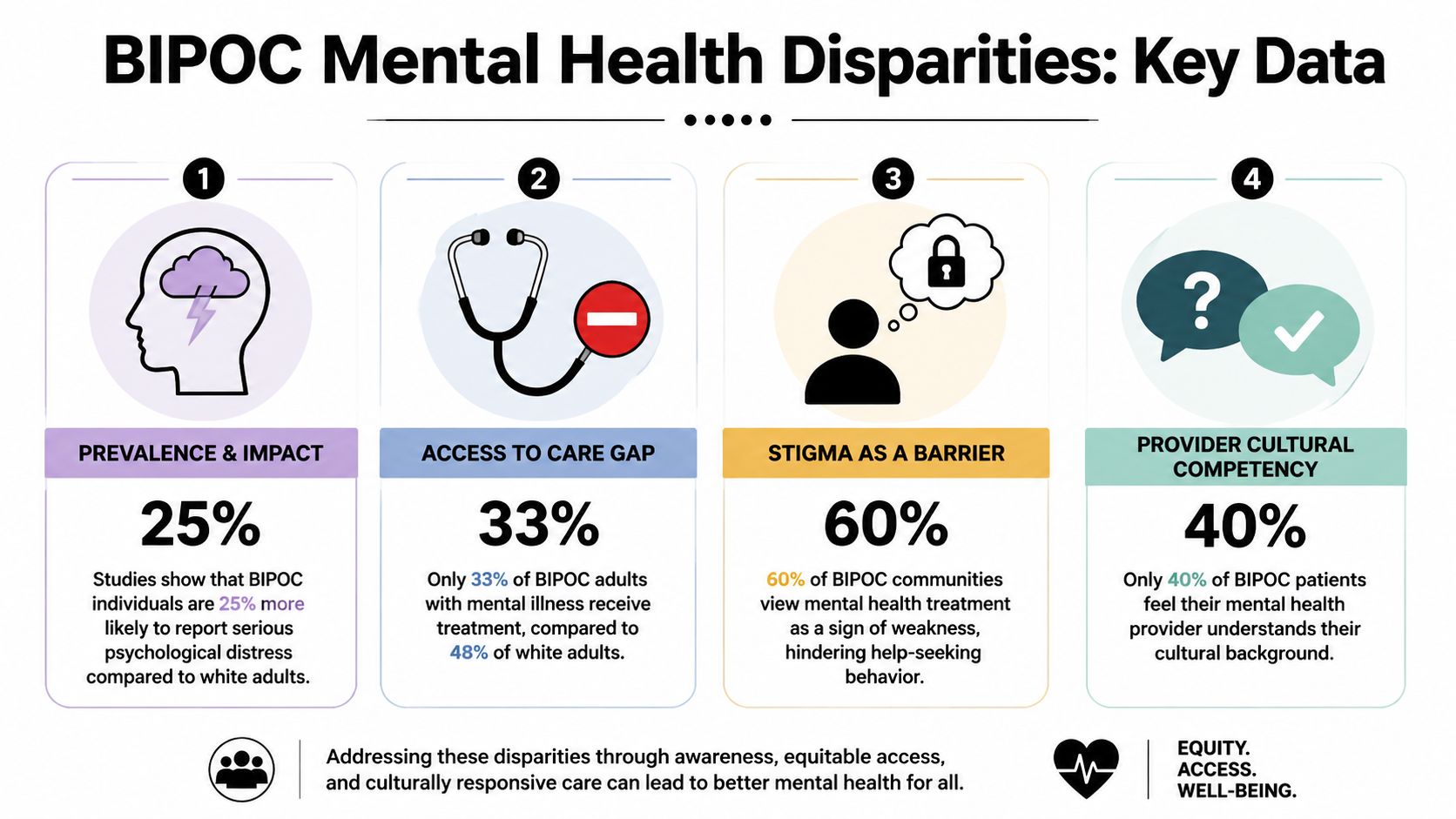
The broad pattern is clear. Need is substantial, and care doesn't reliably follow. Poverty, stigma, discrimination, and mistrust all affect whether symptoms are recognized early, disclosed to professionals, or documented at all.
For lawyers, one practical implication is simple. The absence of a treatment history doesn't tell you the absence of suffering. It often tells you something about access, stigma, and survival strategy.
A simple visual resource like this brain icon reference for mental health materials can also help firms build intake guides or client education sheets that normalize discussion of symptoms without turning the first meeting into a clinical interrogation.
{kind=link}
Why these disparities change legal work
Legal teams often expect clients to come in with records, diagnoses, and prior treatment. That expectation fits some cases. It doesn't fit many BIPOC immigrant clients.
A client may have obvious symptoms but no prior therapy. Another may have sought help only through faith leaders, family, or self-management. Those aren't side notes. They shape how much corroboration exists at intake and whether the attorney needs to proactively obtain a forensic psychological evaluation.
Untreated distress often creates the very inconsistencies that legal teams later struggle to explain.
That is why disparity data isn't just background education. It should change case strategy. It should affect interview pacing, how you assess credibility issues, and whether you treat missing records as a gap to investigate rather than a weakness to concede.
The Compounded Trauma of BIPOC Immigrants

For many BIPOC immigrants, trauma doesn't come from one event. It accumulates across stages. What happened before migration may include racial persecution, community violence, political targeting, trafficking, domestic abuse, or chronic deprivation. The journey itself may involve exploitation, family separation, assault, or prolonged fear. After arrival, detention, instability, anti-immigrant hostility, and racism can keep the nervous system in a constant state of threat.
Trauma rarely begins at the border
In clinical work, this layering matters because it changes presentation. Someone with repeated trauma may not react the way a lawyer expects from a single-incident victim. They may detach, minimize, become highly vigilant, or struggle to identify which experience affected them most. Some clients speak clearly about practical losses while avoiding emotional content altogether.
That pattern is often misread. Attorneys may assume the client is withholding information or doesn't understand what matters legally. In reality, the client may be describing trauma the only way they can tolerate.
According to Steinberg Institute's discussion of barriers to BIPOC mental health services, 68% of BIPOC asylum seekers exhibit PTSD symptoms from pre- and post-migration stressors. The same source states that only 12% of USCIS-approved psychological reports for VAWA cases in FY2024 incorporated BIPOC-specific cultural formulations.
That second point is especially important. A report can be technically competent and still incomplete if it ignores how race, migration history, language, community norms, and distrust of institutions shape symptom expression.
Why cultural formulation matters
A culturally responsive evaluation doesn't invent a diagnosis. It clarifies context. It explains why a client may have delayed care, why they use nonclinical language for severe symptoms, or why family and community pressures affect disclosure.
Here is a useful teaching tool for staff trainings:
When legal teams understand compounded trauma, they stop forcing clients into narrow storytelling models. They build declarations with more patience, they corroborate symptoms more thoughtfully, and they identify earlier when expert mental health evidence is necessary.
Adopting a Trauma-Informed Legal Framework
A trauma-informed framework doesn't require attorneys to act as therapists. It requires them to stop practicing as if testimony comes from a neutral emotional state.
Safety and predictability in the legal setting
Start with the environment. Psychological safety in a law office is practical, not abstract. Clients need to know who will be in the room, how long the meeting will last, whether an interpreter will attend, what topics may be difficult, and whether they can ask for a break.
Predictability matters because trauma reduces tolerance for uncertainty. If your office regularly changes interviewers, reschedules at the last minute, or opens with graphic questioning, clients may shut down or offer the shortest possible answers.
Use simple habits:
- Preview the agenda: Tell the client what today's meeting will cover before questions begin.
- Name the purpose of difficult topics: Explain why details matter legally, especially when asking about abuse, coercion, or past threats.
- Offer choice where possible: Let the client decide whether to start with family history, timeline, or current symptoms.
- Build in pauses: After painful disclosures, stop and orient. Don't immediately jump to cross-examination style clarification.
Collaboration over extraction
Many legal interviews feel extractive. The office needs facts, dates, names, and inconsistencies resolved. Trauma-informed work still gets those facts, but it does so collaboratively.
Data from the Department of Defense work-life campaign PDF discussing BIPOC mental health barriers and self-management notes that 43% of Black and 47% of Hispanic individuals self-manage mental health challenges without therapy. The same source points to tools like the Cumulative Trauma Scale for mapping chronic exposure to oppression into clinical outcomes such as Complex PTSD in legal contexts.
That has two implications for lawyers. First, some clients won't arrive with prior treatment records because self-management has been their norm. Second, repeated trauma may be better understood through cumulative assessment rather than a narrow search for one defining event.
Ask, "What made it hardest to function?" before asking, "What was the worst thing that happened?"
That question often yields better legal detail. It ties experience to impairment, which is where psychological evidence becomes especially useful in hardship and protection-based cases.
Actionable Steps for Your Firm This July
Good intentions fail when they aren't operationalized. July is the right time to assign responsibility, update scripts, and tighten referral criteria.
Culturally responsive outreach
If your firm publishes a July awareness post, make it useful. Don't stop at awareness language. Include signs that stress or trauma may affect memory, sleep, concentration, or disclosure. Clarify that seeking a psychological evaluation for legal purposes isn't a sign of weakness and doesn't mean a client is "crazy." That single clarification removes a lot of resistance.
Outreach should also reflect the communities you serve. Translate core materials. Review whether your examples center only one cultural experience. If your intake staff use community webinars, flyers, or partner presentations, include plain explanations of what a forensic psychological evaluation does and does not do.
A clean visual asset can help standardize branded outreach, such as this practice logo resource for client education materials.
{kind=link}
Integrating mental health screening
You don't need to diagnose clients in-house. You do need a screening habit.
Use brief intake prompts that open the door without forcing disclosure:
- Functioning prompt: "Since these events happened, what has changed in your sleep, concentration, work, or parenting?"
- Avoidance prompt: "Are there parts of your story that feel hard to talk about even when you want to explain them?"
- Safety prompt: "Do certain reminders cause panic, numbness, or a need to leave the room?"
- Care history prompt: "Have you ever wanted help for stress, fear, or sadness but felt unable to get it?"
These questions surface impairment. They also help you decide whether a formal evaluation could strengthen the case.
Building a referral network
Not every clinician is suited for immigration work. Vet for forensic writing skill, cultural responsiveness, interpreter experience, virtual capacity, and familiarity with PCL-5 or other established trauma assessment tools when appropriate to the case.
The disparity remains significant. As noted earlier, treatment access for Black adults lags well behind white adults. In legal practice, that means a culturally competent evaluator may need to document why care was delayed and how mistrust or poverty affected treatment history, rather than treating the lack of treatment as clinically neutral.
A useful referral network usually includes:
- One evaluator for urgent filing timelines
- One evaluator comfortable with severe trauma presentations
- One backup option for language or scheduling constraints
- At least one provider able to work remotely in a HIPAA-compliant format
Reinforcing confidentiality and HIPAA practices
Clients often withhold information because they don't understand where it will go. Explain confidentiality early and repeat it before sensitive interviews. Distinguish between what stays within the legal team, what may appear in filings, and what requires the client's informed consent.
This matters even more when families are involved. A spouse, parent, or adult child may want to sit in on an intake, but their presence can suppress disclosure about abuse, coercion, sexuality, or trauma symptoms. Build a policy for part of every intake to occur privately.
Mastering trauma-informed interviewing
The interview itself is where many firms either build trust or lose it. Slow down your sequence.
Use grounding tactics when a client becomes overwhelmed. Ask what they notice in the room. Offer water. Shift briefly to neutral facts. Then decide whether to continue, pause, or schedule a follow-up.
Here is a practical framework your staff can implement:
| Action Area | Specific Step | Tool or Resource Example |
|---|---|---|
| Intake | Add four mental health screening prompts to the first substantive meeting | Standardized intake form |
| Referrals | Create a shortlist of culturally responsive forensic evaluators | Referral tracker with language capacity |
| Client education | Explain what a psychological evaluation can document in immigration cases | One-page handout |
| Interviewing | Build scheduled breaks into trauma-heavy meetings | Interview checklist |
| Confidentiality | Review privacy rules before sensitive disclosures | Written consent and privacy script |
Building a Supportive Ecosystem Beyond Your Firm
A single firm can improve its internal process. A local network can improve outcomes at scale.
Partnerships that improve both care and evidence
The best partnerships are concrete. Work with community centers, immigrant advocacy groups, shelters, survivor organizations, and clinicians who understand both trauma and the immigration system. Co-host short July trainings on topics like trauma and memory, preparing for psychological evaluations, or how mental health evidence fits asylum and VAWA cases.

The case value is measurable. According to Magellan Health Insights on improving mental health during BIPOC Mental Health Awareness Month, asylum cases with BIPOC applicants supported by psychological evaluations have 32% higher approval rates, yet only 18% of BIPOC U Visa filings include such reports. The same source states that FY2025 USCIS updates prioritize trauma-informed evidence, with BIPOC Extreme Hardship Waiver denials dropping 15% when reports address cultural mistrust.
Those figures should push firms beyond passive referral lists. If evaluations improve outcomes but are still underused, the bottleneck is usually operational. Clients don't know what an evaluation is. Attorneys wait too long to refer. Community partners don't know when a legal case would benefit from clinical documentation.
A useful explainer for partner orientation can sit alongside a simple about page image for practice introductions in webinar decks or referral packets.
{kind=link}
Community education works best when legal and mental health partners use the same language for timing, confidentiality, and evidentiary purpose.
Set goals that change case preparation
Awareness campaigns are forgettable unless they change behavior. Set goals tied to actual workflow.
For example:
- Referral timing: Track whether potential evaluation cases are identified early enough to avoid rushed filings.
- Screening consistency: Audit whether intake staff are using the same mental health prompts across offices.
- Partner responsiveness: Review which clinicians can meet filing deadlines and produce legally useful reports.
- Client support: Monitor whether referred clients connect with evaluators or drop off after the first handoff.
Firms don't need elaborate dashboards. They need accountability. One designated attorney or senior paralegal can review July referrals, identify preventable delays, and adjust the process before those problems affect fall filings.
From Awareness to Action A Commitment to Your Clients
BIPOC mental health month should change how immigration lawyers practice, not just what they post. The deeper lesson is straightforward. Many BIPOC immigrant clients carry trauma that is cumulative, culturally shaped, and underdocumented. If a firm ignores that reality, it may misread the client and weaken the case.
A better approach is available. Build predictable interviews. Screen for impairment early. Refer to culturally responsive evaluators when the record needs clinical context. Explain confidentiality clearly. Train staff to recognize that delayed disclosure and fragmented memory often reflect trauma rather than unreliability.
These changes support both ethics and outcomes. They help clients feel safer telling the truth, and they help attorneys present that truth in a form USCIS and the immigration courts can understand.
The strongest firms treat July as a checkpoint, not a campaign. They use bipoc mental health month to improve systems that will still matter in October, January, and every urgent filing season after that.
If your firm needs immigration-focused psychological evaluations that are evidence-based, trauma-informed, and built for legal usefulness, Pro Psychological Analysis provides assessments for asylum, T visa, U visa, VAWA, and extreme hardship cases. The practice works with attorneys to document trauma, abuse dynamics, and clinically significant symptoms in clear, admissible reports while protecting client dignity through HIPAA-compliant, confidential care.